
Vol 1, No 1 (2025): Current Issue (Volume 1, Issue 1), 2025
Original Article
Hyalinizing Trabecular Tumor: A Case Series with Literature Review
Abdulwahid M. Salih, Rebaz O. Mohammed, Hiwa O. Baba, Shko H. Hassan, Muhammed Bag A. Ali, Imad...
Abstract
Introduction: Hyalinizing trabecular tumor (HTT) is a rare thyroid neoplasm originating from follicular cells and poses diagnostic challenges due to its cytologic and histologic overlap with other thyroid malignancies. This study aims to present the clinical features and management of HTT cases treated at a single center.
Methods: This was a single-center retrospective case series. The patients were included from January 2019 to November 2024. Data collection took place over one month, from November 15, 2024, to December 15, 2024. The study included patients with HTT whose diagnoses were confirmed histopathologically.
Results: The case series included 11 patients, predominantly female, 10 (90.9%), with a mean age of 50.7±19.01 years. The most common presenting symptom was anterior neck swelling, recorded in 5 (45.5%), while one case (9.1%) was discovered incidentally. Hyperthyroidism was present in 6 (54.5%). The tumors were distributed within the thyroid gland as follows: left lobe in 5 (45.5%) cases, right lobe in 4 (36.4%) cases, and isthmus in 2 (18.1%) cases. Total thyroidectomy was performed in 7 patients (63.6%), with tumor sizes ranging from 0.5 to 5.5 cm and a mean diameter of 2.6 ± 2.05 cm. All diagnoses were confirmed postoperatively through histopathological examination.
Conclusion: A rare benign tumor, HTT remains challenging to diagnose accurately. Both total thyroidectomy and lobectomy may result in good outcomes.
Introduction
Thyroid neoplasms include a wide range of lesions with varying behavior and prognosis [1]. They are generally classified as benign, low-grade malignant, or malignant. Benign tumors, such as adenomas, are common and usually do not cause symptoms. Low-grade malignant neoplasms, like follicular thyroid carcinoma, tend to be more aggressive but often have a good prognosis [2]. Hyalinizing trabecular tumor (HTT) of the thyroid was first identified in 1987. It accounts for approximately 1% of all thyroid tumors, occurs six times more often in men than women, and is most frequently diagnosed in individuals in their 50s [3]. HTT was originally classified as a variant of follicular adenoma but is frequently misdiagnosed due to overlapping morphological features with several thyroid neoplasms. These include papillary thyroid carcinoma (PTC) and medullary thyroid carcinoma. Diagnostic challenges also extend to rare tumors with trabecular architecture, such as fetal-type follicular adenoma, poorly differentiated carcinoma, intrathyroid parathyroid neoplasms, and metastatic lesions to the thyroid [4,5]. This poses a challenge in the clinical management of these lesions, as an accurate presurgical diagnosis of HTT is essential to prevent unnecessary overtreatment of this tumor. A literature review reveals that an accurate preoperative cytological diagnosis of HTT was made in only 8% of reported cases. More worrisome, however, is that the remaining 92% were misdiagnosed with false-positive results [6].
The classification of HTT as benign or malignant remains controversial. While it is generally regarded as benign, it is considered a borderline tumor with the potential for malignancy [7]. This diagnostic complexity has led to confusion in terminology, with HTT also being referred to by various other names, including hyalinizing trabecular adenoma, paraganglioma-like adenoma, hyalinizing trabecular neoplasm, and hyalinizing trabecular carcinoma [8]. This study aims to provide a comprehensive overview of HTT by retrospectively analyzing 11 cases, focusing on clinical presentations, diagnostic challenges, and treatment outcomes.
Methods
Study design
This study was a retrospective single-center case series. The patients were managed over five years, from January 2019 to November 2024. Data collection took place over one month, from November 15, 2024, to December 15, 2024. This study was approved by the Ethics Committee of Kscien organization (Approval No. 2025-33).
Participants
The study included all patients diagnosed with hyalinizing trabecular tumor. Diagnoses were confirmed through histopathological examination of resected thyroid tissue. Clinical and sociodemographic data were collected from patients, medical records, and healthcare providers.
Pre-intervention assessment
Assessments included vital signs monitoring, ultrasonography (U/S), thyroid function tests, serum calcium levels, vocal cord evaluation, viral screening (HBV, HCV, and HIV), and complete blood count.
Intervention
All patients underwent surgery under general anesthesia and were positioned supine with the neck extended and elevated using a roller placed beneath the shoulders. If visible, a 4 cm transverse collar incision was made in a natural skin crease of the lower neck for cosmetic purposes. Subplatysmal flaps were elevated superiorly and inferiorly to allow adequate thyroid gland exposure. A circular skin flap was then raised, with dissection carried laterally, medially, and toward the upper and lower cervical regions.
The midline between the strap muscles was divided, and the muscles were retracted laterally to expose the thyroid gland. Dissection commenced with ligation of the middle thyroid vein, followed by the superior and inferior pedicles. The superior and inferior thyroid vessels were ligated and divided close to the thyroid capsule to preserve the recurrent laryngeal nerves and avoid compromising the parathyroid gland vasculature. To minimize thermal injury, electrocautery use was limited; instead, multiple suture ligatures were applied to control oozing. Both sharp and blunt dissection techniques were employed to identify and preserve the recurrent laryngeal nerves, with all dissections maintained close to the thyroid capsule. The parathyroid glands were preserved in all cases, and surrounding adipose tissue was retained to maintain vascular integrity. In cases where devascularization was suspected, parathyroid autotransplantation into the sternocleidomastoid muscle was performed.
Of the 11 patients, 7 underwent total thyroidectomy. One of these patients underwent additional lateral and central neck dissection, with identification and preservation of the internal jugular vein, spinal accessory nerve, and phrenic nerve. The remaining 4 patients underwent lobectomy, performed using the same surgical technique but limited to the involved thyroid lobe.
After each procedure, hemostasis was confirmed. Closed suction drains (RediVac®) were placed in the patients. The strap muscles were reapproximated in the midline, and the skin was closed with absorbable subcuticular sutures and Steri-Strips. All patients tolerated the procedure without intraoperative complications.
Post-intervention Considerations
Postoperatively, all patients received intravenous paracetamol, and those who underwent total thyroidectomy were prescribed thyroid hormone replacement therapy (Levothyroxine) adjusted to their body weights. The diagnosis was confirmed through histopathological examination of the surgical specimens.
Results
Participants
The case series included 11 patients, of whom ten (90.9%) were female. Patient ages ranged from 32 to 85 years, with a mean age of 50.7±19.01 years. Seven patients (63.6%) had no significant past medical history, while three (27.3%) had hypertension, including one with concurrent type 2 diabetes and another with a history of renal stones. Surgical history was positive in six patients (55.5%). The most common presenting symptom was anterior neck swelling, observed in six patients (54.5%), followed by weight loss in three patients (27.3%). In one case (9.1%), the finding was incidental. Preoperative thyroid function assessment revealed hyperthyroidism in six patients (54.5%), and the remaining five (45.5%) were euthyroid (Table 1).
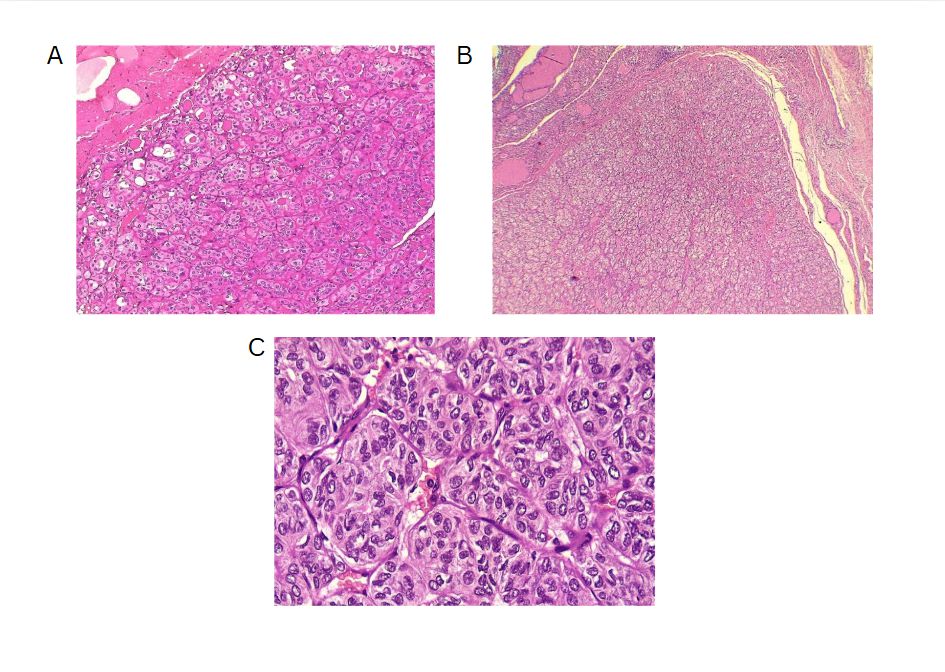
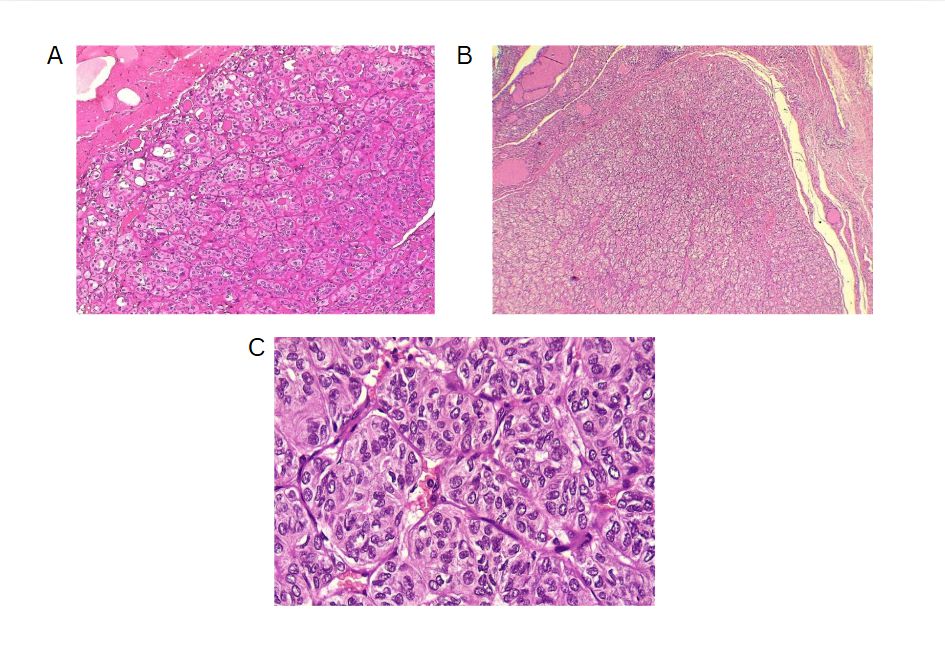
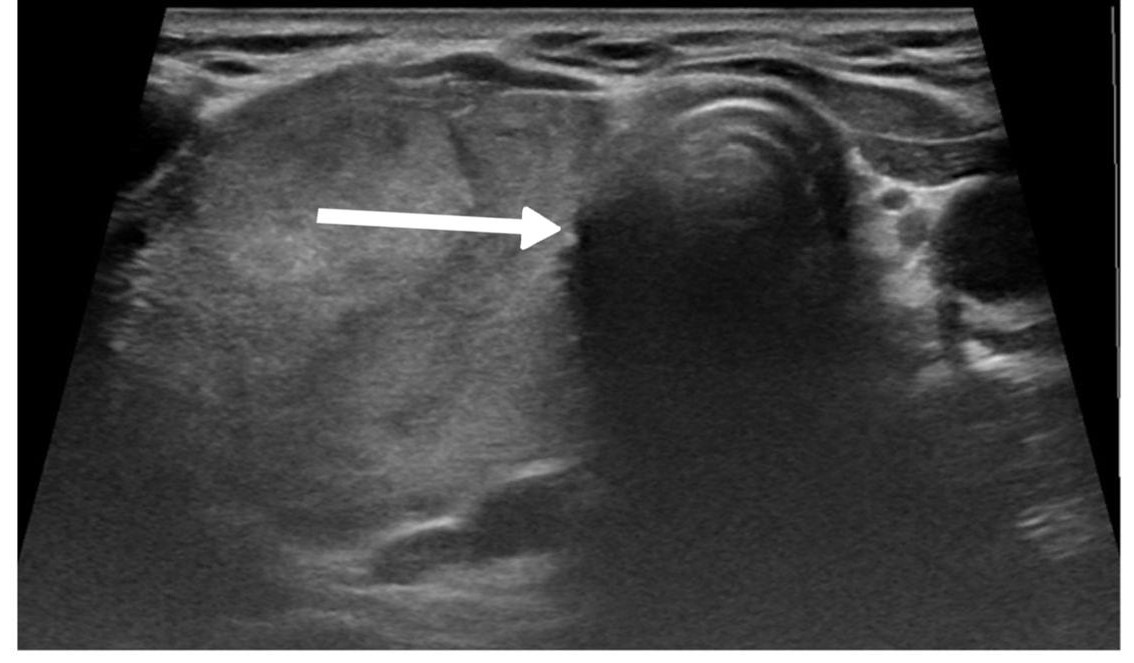
The left thyroid lobe was involved in five cases (45.5%), the right lobe in four cases (36.4%), and the isthmus in two cases (18.1%). The primary surgical approach was total thyroidectomy in seven cases (63.6%), including one patient who underwent concurrent neck dissection (Table 2). Tumor size ranged from 0.5 to 5.5 cm, with a mean size of 2.6 cm (Table 3). All the diagnoses were made post-operatively through histopathological examination (Figure 1).
Outcomes and follow-up
The follow-up period ranged from one month to five years, with a mean duration of 2.3±1.27 years. During this period, no cases of recurrence were reported, and all patients achieved complete recovery. No significant complications were observed during or after the surgical procedures.
|
Case no. |
Age |
Sex |
Medical history |
Surgical history |
Drug history |
Chief complaint |
Duration |
Examination |
Thyroid function test |
|
1 |
39 |
F |
Unremarkable |
Unremarkable |
Unremarkable |
Incidental |
1 week |
Not palpable |
Hyperthyroid |
|
2 |
78 |
F |
Hypertension |
Cataract surgery & cholecystectomy |
Statin, Anticoagulant & Anti-Hypertension |
Shortness of breath |
8 years |
Hard |
Hyperthyroid |
|
3 |
74 |
M |
Unremarkable |
Kidney transplant |
Corticosteroids |
Weight-loss |
5 months |
Not palpable |
Hyperthyroid |
|
4 |
85 |
F |
Hypertension & renal stone |
Thyroid lobectomy & lithotripsy |
Anti-Hypertension |
Anterior neck swelling |
6 years |
Hard |
Euthyroid |
|
5 |
32 |
F |
Unremarkable |
Unremarkable |
Unremarkable |
Anterior neck swelling |
3 months |
Hard |
Euthyroid |
|
6 |
34 |
F |
Hodgkin’s lymphoma |
C-section & cervical cerclage |
Antibiotics |
Weight-loss |
8 months |
Not palpable |
Euthyroid |
|
7 |
38 |
F |
Unremarkable |
Cholecystectomy |
Unremarkable |
Anterior neck swelling |
1.5 years |
Hard |
Hyperthyroid |
|
8 |
42 |
F |
Unremarkable |
Unremarkable |
Unremarkable |
Anterior neck swelling |
1 year |
Hard |
Euthyroid |
|
9 |
51 |
F |
Hypertension & Type 2 Diabetes Mellitus |
Unremarkable |
Anti-Hypertension & Anti-diabetics |
Anterior neck swelling |
2 months |
Hard |
Hyperthyroid |
|
10 |
40 |
F |
Unremarkable |
Unremarkable |
Unremarkable |
Weight-loss |
6 months |
Not palpable |
Euthyroid |
|
11 |
45
|
F |
Unremarkable |
Unremarkable |
Unremarkable |
Anterior neck swelling |
1 year |
Hard |
Hyperthyroid |
|
M:Male, F:Female, S.Ca:Serum calcium, TG:Thyroglobulin, N/A:Not applicable |
|||||||||
|
Case no. |
S. Ca (mg/dL) |
US |
US consistency |
US echogenicity |
Side |
FNA Bethesda |
Vocal cord assessment |
Type of operation |
Post Op complications |
HPE |
Tumor Size (cm) |
Follow-up (years) |
|
1 |
N/A |
N/A |
N/A |
N/A |
Left lobe |
V |
Normal |
Lobectomy |
None |
HTT |
1.4 |
5 |
|
2 |
9.6 |
TR3 |
Mixed |
Heterogenous |
Left lobe |
IV |
Normal |
Total thyroidectomy |
None |
HTT |
3.8 |
2 |
|
3 |
7.9 |
GD |
No nodule |
No nodule |
Isthmus |
NP |
Normal |
Total thyroidectomy |
None |
HTT |
1 |
2 |
|
4 |
9.8 |
GD |
No nodule |
No nodule |
Right lobe |
NP |
Normal |
Total thyroidectomy |
None |
HTT |
6 |
0.08 |
|
5 |
9.2 |
TR4 |
Solid |
Hyperechoic |
Left lobe |
V |
Normal |
Total thyroidectomy |
None |
HTT |
4.5 |
3 |
|
6 |
9.5 |
TR4 |
Solid |
Hyperechoic |
Left lobe |
V |
Normal |
Total thyroidectomy |
None |
HTT |
0.5 |
3 |
|
7 |
9.1 |
TR3 |
Solid |
Heterogenous |
Left lobe |
NP |
Normal |
Lobectomy |
None |
HTT |
1.4 |
1 |
|
8 |
9.5 |
TR4 |
Solid |
Hypoechoic |
Right lobe |
IV |
Normal |
Lobectomy |
None |
HTT |
3 |
2 |
|
9 |
9 |
TR3 |
N/A |
N/A |
Isthmus |
NP |
Normal |
Total thyroidectomy |
None |
HTT |
0.8 |
2 |
|
10 |
9.2 |
TR3 |
N/A |
N/A |
Right lobe |
III |
Normal |
Total thyroidectomy |
None |
HTT |
0.7 |
3 |
|
11 |
8.9 |
TR3 |
N/A |
N/A |
Right lobe |
NP |
Normal |
Lobectomy |
None |
HTT |
5.5
|
3
|
|
N/A: Not Applicable, S.Ca: Serum Calcium, US: Ultrasound, FNA: Fine Needle Aspiration, OP: Operation, HPE: Histopathology, TR: TI-RADS, GD: Graves' Disease, NP: Non-Productive, HTT: Hyalinizing trabecular tumor |
||||||||||||
|
Variables |
Frequency |
|
Sex |
|
|
Male |
1 (9.1%) |
|
Female |
10 (90.9) |
|
Age groups (years) |
|
|
30-39 |
4 (36.3%) |
|
40-49 |
3 (27.3%) |
|
50-59 |
1 (9.1%) |
|
>60 |
3 (27.3%) |
|
Mean ± SD |
50.7 ± 19.0 |
|
Medical history |
|
|
Unremarkable |
7 (63.6%) |
|
Hypertension |
1 (9.1%) |
|
Hypertension & renal stones |
1 (9.1%) |
|
Hodgkin’s lymphoma |
1 (9.1%) |
|
Hypertension & Type 2 Diabetes Mellitus |
1 (9.1%) |
|
Surgical history |
|
|
Unremarkable |
6 (54.5%) |
|
Cholecystectomy |
1 (9.1%) |
|
C-section & cervical cerclage |
1 (9.1%) |
|
Cholecystectomy & cataract surgery |
1 (9.1%) |
|
Kidney transplant |
1 (9.1%) |
|
Thyroid lobectomy & lithotripsy |
1 (9.1%) |
|
Drug history |
|
|
Negative |
6 (54.5%) |
|
Corticosteroids |
1 (9.1%) |
|
Antibiotics |
1 (9.1%) |
|
Antihypertensive |
1 (9.1%) |
|
Antihypertensive & Antidiabetic |
1 (9.1%) |
|
Chief complaint |
|
|
Anterior neck swelling |
6 (54.5%) |
|
Shortness of breath |
1 (9.1%) |
|
Weight loss |
3 (27.3%) |
|
Incidental |
1 (9.1%) |
|
Thyroid examination |
|
|
Not palpable |
7 (63.6%) |
|
Hard |
4 (36.4%) |
|
Thyroid function |
|
|
Hyperthyroid |
6 (54.5%) |
|
Euthyroid |
5 (45.5%) |
|
Affected side |
|
|
Right lobe |
4 (36.3%) |
|
Left lobe |
5 (45.5%) |
|
Isthmus |
2 (18.2%) |
|
Operation |
|
|
Total thyroidectomy |
7 (63.6%) |
|
Lobectomy |
4 (36.4%) |
|
Tumor size (cm) |
|
|
Mean ± SD |
2.6 ± 1.95 |
|
Follow-up (years) |
|
|
0.0 - 1.0 |
2 (18.18%) |
|
1.1 - 2.0 |
4 (36.36%) |
|
2.1 - 3.0 |
4 (36.36%) |
|
3.1 - 4.0 |
0 (0.0%) |
|
4.1 - 5.0 |
1 (9.09 %) |
|
Mean ± SD |
2.3 ± 1.27 |
Discussion
The diagnosis of HTT is challenging due to its resemblance to other thyroid neoplasms. While most cases are asymptomatic, Rossi et al. stated that symptom presentation may depend on tumor size and location [5]. Among the 11 cases, only one was asymptomatic, while the remaining ten exhibited clinical symptoms, including anterior neck swelling, weight loss, and shortness of breath. However, in the six reviewed cases, three were asymptomatic, two exhibited neck swelling, and one experienced both dyspnea and dysphagia (Table 4) [2,3,7-10].
|
Author/year |
Age |
Sex |
Medical history |
Drug history |
Surgical history |
Chief complaint |
Examination |
Duration (years) |
Side
|
Size (cm)* |
Distant metastasis |
TI-RADS |
FNA findings |
Therapeutic approach |
IHC findings |
Diagnosis |
Outcome |
Follow-up (years) |
|
Zhang et al./2025 [7] |
31 |
F |
Unremarkable |
Unremarkable |
Unremarkable |
Incidental |
Palpable mass |
1.5 |
R |
2.2 |
No |
TR3 |
N/A |
Lobectomy |
TG +ve, CK19 +ve, TTF-1 +ve & Ki-67 5% |
HTT |
Resolved |
0.6 |
|
Hayashi et al./2025 [2] |
93 |
F |
Diabetes mellitus, hyperlipidemia, hypertension & myocardial infarction |
N/A |
N/A |
Loss of appetite, dyspnea & dysphagia |
Enlarged, firm, non-tender, without palpable nodules |
>12 |
B |
>10 |
No |
N/A |
N/A |
Conservative management & rehabilitation |
N/A |
HTT |
Improved |
N/A |
|
Alsogair et al./2023 [3] |
60 |
M |
Unremarkable |
Unremarkable |
Hemorrhoidectomy |
Mass on the neck |
Palpable, firm & non-tender |
N/A |
R |
3.8 |
No |
N/A |
60%-75% likelihood of malignancy |
Total thyroidectomy followed by thyroxine |
TG +ve & Ki-67 +ve |
HTT |
Resolved |
0.06 |
|
Katano et al./ 2021 [10] |
54 |
F |
Panic disorder & chronic thyroiditis |
Unremarkable |
Unremarkable |
Left cervical mass |
Growing, painless & elastic |
N/A |
L |
4.5 |
No |
N/A |
Chronic thyroiditis with possible malignancy |
Lobectomy |
Ki-67 +ve for cytoplasm & ColIV +ve |
HTT |
Resolved |
1.5 |
|
Rhee et al./2018 [9] |
63 |
F |
Breast cancer |
N/A |
N/A |
Incidental |
N/A |
N/A |
L |
0.6 |
No |
N/A |
Features of PTC |
Lobectomy |
Ki-67 +ve, CD56 +ve & Galectin-3 +ve |
HTT |
Resolved |
N/A |
|
Jones et al./2017 [8] |
70 |
F |
N/A |
N/A |
N/A |
Incidental |
N/A |
N/A |
R |
1.94 |
N/A |
N/A |
60-75% likelihood of malignancy |
Total thyroidectomy |
TG +ve, vimentin +ve & CK19 +ve |
HTT |
Resolved |
0.08 |
|
M: Male, F: Female, N/A: Not applicable, FNA: Fine needle aspiration, IHC: Immunohistochemistry, HTT: Hyalinizing trabecular tumor, L: Left, R: Right, B: Both |
||||||||||||||||||
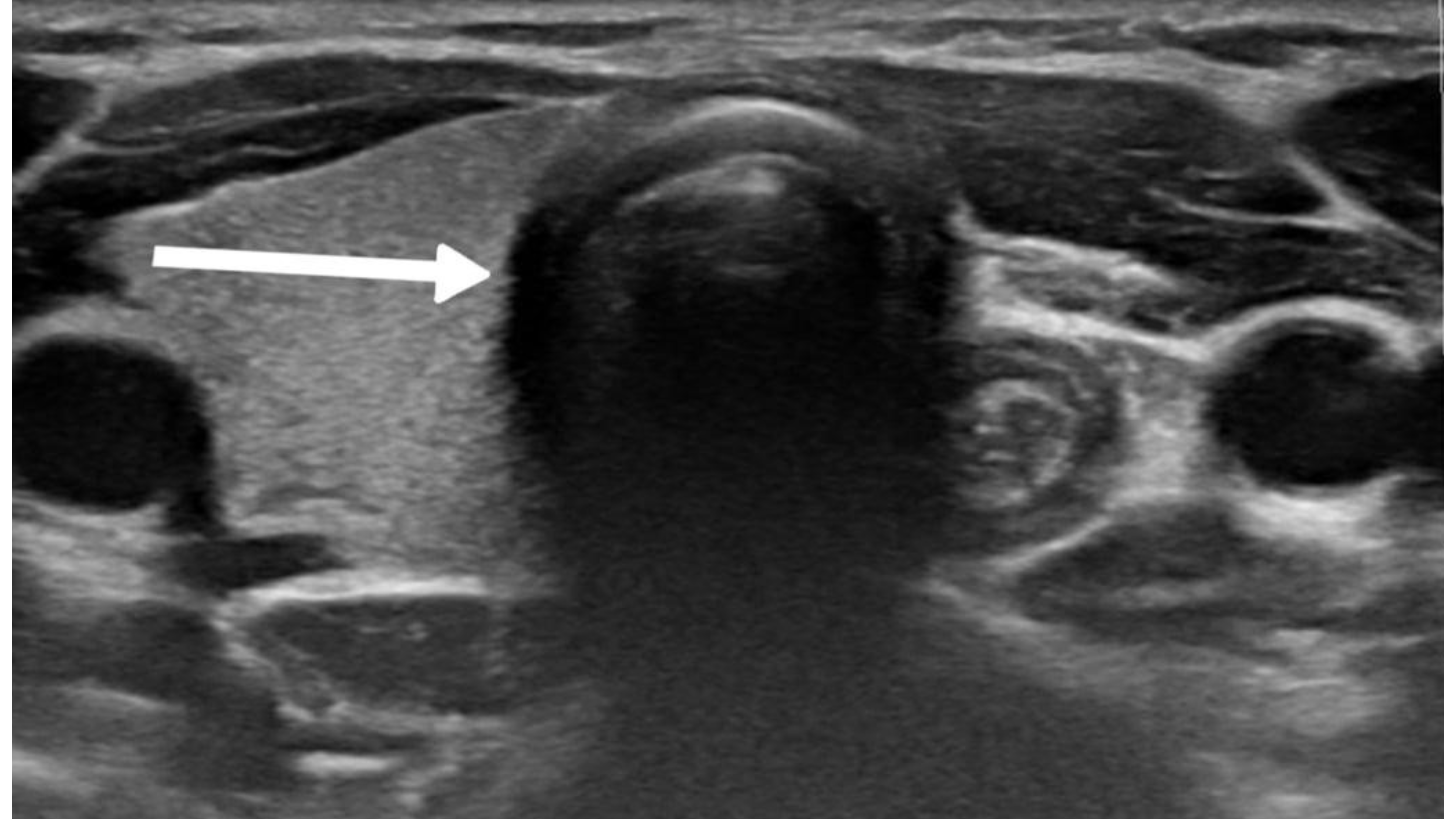
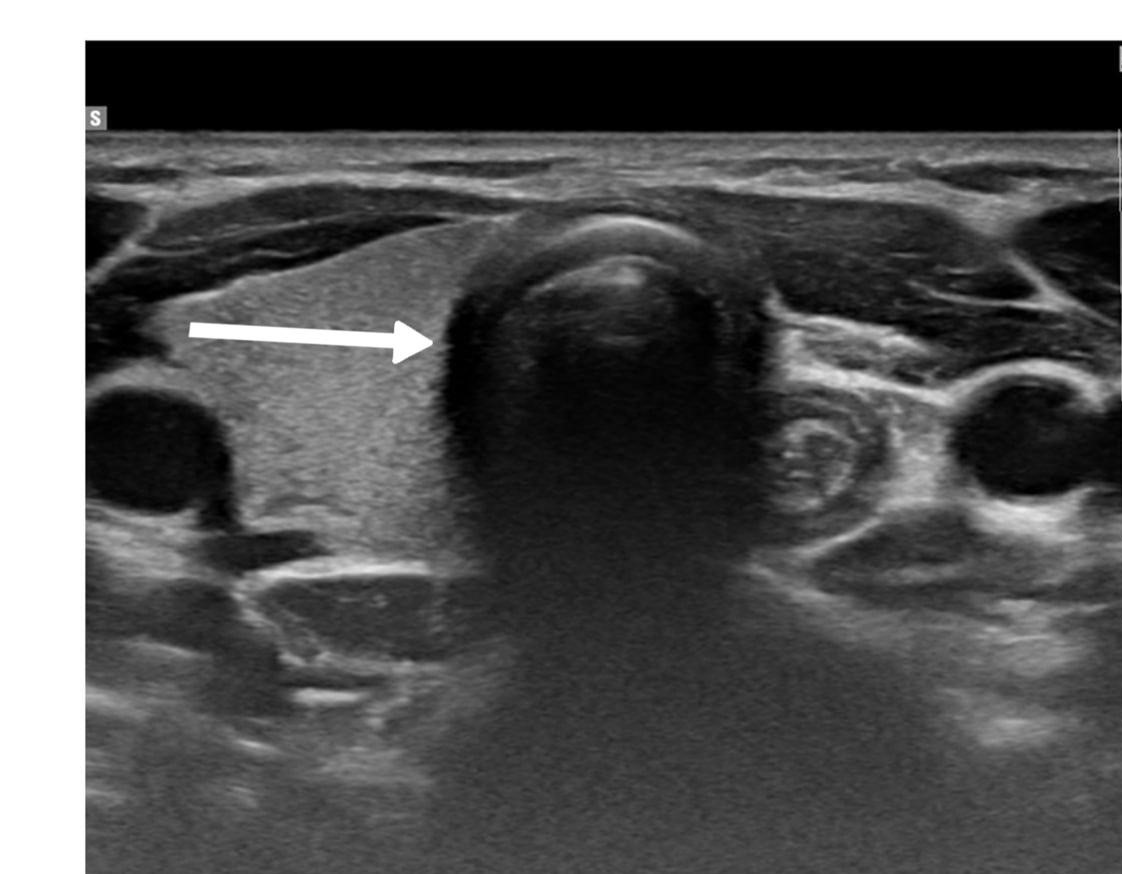
The diagnostic evaluation of most thyroid nodules typically begins with U/S, followed by fine needle aspiration (FNA). The U/S findings suggestive of HTT are well-defined, solitary, oval or round, solid hypoechoic nodules, usually without microcalcifications and displaying peri or intra-nodular vascularity. However, these features are not specific to HTT and may also occur in other thyroid lesions [7]. Recognizing the variability in U/S findings is crucial, as some studies reported an absence of malignant features. In contrast, Choi et al. found that 29% of HTT cases displayed malignant features on U/S [5,11]. In the present study, five cases were classified as mildly suspicious for malignancy, and three were considered moderately suspicious for malignancy according to the thyroid imaging reporting and data system (TI-RADS). Among the reviewed cases, malignancy was also suspected in four patients based on the U/S findings [2,3,7-10].
The primary diagnostic tool for thyroid nodules is FNA, which often leads to the misclassification of HTT as PTC or medullary thyroid carcinoma [9]. Ito et al. suggested that this diagnostic confusion arises from shared cytological features, including intranuclear cytoplasmic inclusions and nuclear grooves, which represent hallmark characteristics of PTC [4]. The cytological appearance of HTT on liquid-based preparations reveals cohesive aggregates or syncytial fragments of tumor cells surrounding hyaline material. Although tumor cells in HTT show enlarged nuclei with hyperchromasia and occasional intranuclear pseudo-inclusions similar to papillary carcinoma, HTT cells typically display dispersed fine chromatin rather than the pale and clear chromatin pattern observed in PTC [9].
Additionally, HTT cells demonstrate less frequent nuclear membrane irregularity and exhibit a more stratified trabecular arrangement compared to papillary carcinoma. These subtle distinctions prove crucial for accurate cytological interpretation, though they remain challenging to discern consistently in clinical practice [9]. Dell’Aquila et al. reported that up to 75% of HTTs are classified within Bethesda categories IV to VI [12]. Among the cases included, two were diagnosed as Bethesda category IV, while three were classified as category V, emphasizing their frequent misinterpretation by cytopathologists. Equivocal cytomorphologic diagnoses, such as atypia of undetermined significance or follicular lesion of undetermined significance, require repeat FNA, as the malignancy risk for nodules in these categories ranges from 1% to 15% [8].
On gross examination, HTT typically presents as a solid, well-circumscribed mass, or less commonly, as an encapsulated tumor, with colors ranging from yellow to tan, opposite to PTC, which is usually white and does not have a capsule. HTT generally lacks invasion into the capsule, vasculature, or thyroid parenchyma [5,7]. However, Gowrishankar reported a case in which invasion and malignant behavior were observed in HTT [13].
Immunohistochemistry can aid in diagnosing HTT, although some biomarkers used may lack significant specificity. HBME-1 and galectin-3 are well-established markers for malignant thyroid lesions, particularly PTC and its variants. However, their expression in HTT
remains a subject of debate. In their series, Dell’Aquila et al. found that the majority of HTT cases exhibited a distinct immune profile, with negative immunoreactivity observed in 16 out of 18 (89%) lesions. This finding further supports the classification of HTT as a benign tumor [12].
Recent genetic studies have demonstrated that GLIS rearrangements, particularly the PAX8-GLIS3 gene fusion, are critical for diagnosing HTT. Research indicates this fusion was present in 93% of HTT cases (13 out of 14), with the remaining 7% involving a PAX8-GLIS1 rearrangement. These findings highlight the diagnostic utility of detecting GLIS-related fusions to distinguish HTT from morphologically similar thyroid neoplasms [4].
In 2012, Smith et al. suggested that HTT could potentially acquire mutations leading to RET/PTC expression and undergo malignant transformation into PTC [14]. Given the uncertainty regarding the malignant potential of HTT, treatment approaches typically involve complete resection, near-total thyroidectomy, or lobectomy [8]. However, evidence suggests that up to three-quarters of patients may be subjected to overtreatment, opting for total or subtotal thyroidectomy rather than the less invasive lobectomy. In contrast, some experts argue for a more conservative management strategy, advocating for close monitoring or lobectomy as a first-line approach, rather than resorting to total thyroidectomy immediately [8]. Among the cases included in the current series, seven patients underwent total thyroidectomy, accounting for 63.6% of the surgeries performed. Utilizing total thyroidectomy as the surgical method mainly resulted from uncertainty in diagnosis, as imaging and other pre-operative examinations don’t usually provide a solid diagnosis.
Conclusion
In conclusion, HTT is a rare tumor that is challenging to diagnose accurately. Both total thyroidectomy and lobectomy may result in good outcomes.
Declarations
Conflicts of interest: The authors have no conflicts of interest to disclose.
Ethical approval: Ethical approval for this study was obtained from the Ethics Committee of the Kscien Organization (Approval No. 2025-33)
Consent for participation: Not applicable.
Consent for publication: Written informed consent for publication was obtained from all patients.
Funding: The present study received no financial support.
Acknowledgments: None to be declared.
Authors' contributions: AMS, ROM, FHK, and MMA: Major contributors to the conception of the study, as well as the literature search for related studies, and manuscript writing. HOB, SHH, MBA, IJH, ISS, and DQH: Literature review, design of the study, critical revision of the manuscript, and processing of the tables. KKM, MNH, AAQ, HAA, and HKM: Literature review and processing of the figure. All authors have read and approved the final version of the manuscript.
Use of AI: ChatGPT-3.5 was used to assist with language refinement and improve the overall clarity of the manuscript. All content was thoroughly reviewed and approved by the authors, who bear full responsibility for the final version.
Data availability statement: Not applicable.
Thyroid Hemiagenesis: A Single-Center Case Series
Abdulwahid M. Salih, Hiwa O. Baba, Shaho F. Ahmed, Karzan M. Salih, Abdullah A. Qadir, Ayman M....
Abstract
Introduction: Thyroid hemiagenesis (TH) is a rare congenital anomaly characterized by the complete absence of one thyroid lobe, with or without absence of the isthmus. Its etiology remains unclear, and epidemiological data are limited. Although TH is often asymptomatic and discovered incidentally, it may pose clinical challenges when accompanied by thyroid dysfunction or structural abnormalities. This study reviews a single-center experience in diagnosing this condition and highlights its clinical significance..
Methods: This single-center case series was conducted from July 2021–July 2024, analyzing TH cases confirmed via ultrasonography. Eligible patients had complete medical records, including demographics, clinical presentation, radiological findings, and thyroid function status. Data were retrieved from electronic records and analyzed using SPSS 27.0, employing descriptive statistics to summarize means, ranges, frequencies, and percentages, ensuring a comprehensive assessment of TH’s clinical and epidemiological characteristics..
Results: This study analyzed 11 patients with TH (mean age: 28.12 ± 18.14 years; range: <1–55 years), seven of whom were females (63.6%). The diagnosis was incidental in six cases (54.5%), while three (27.3%) presented with neck swelling and two (18.2%) with neck pain. Thyroid function was euthyroid in seven (63.6%), hyperthyroid in two (18.2%), and hypothyroid in two (18.2%). Ultrasound examination confirmed left lobe and isthmus agenesis in eight cases (72.7%). Follow-up ranged from 4 to 48 months.
Conclusion: This study confirms the female predominance of TH, with left-lobe absence being the most common. Congenital anomalies suggest embryological links. While thyroid function is typically preserved, those with hypo- and hyperthyroidism highlight the need for individualized endocrine assessment and monitoring.
Introduction
Thyroid hemiagenesis (TH), first described in 1852, is characterized by the absence of one thyroid lobe, with or without the isthmus. It is typically detected incidentally during neck imaging, as most affected individuals remain asymptomatic and undiagnosed. However, epidemiological studies suggest a higher occurrence in regions endemic for hypothyroidism, potentially indicating an underlying environmental or genetic predisposition [1].
Epidemiological analyses reveal distinct anatomical patterns in TH. Approximately 80% of documented cases involve agenesis of the left thyroid lobe, establishing a left-to-right prevalence ratio of 4:1. When the left lobe is absent, the isthmus is missing in nearly half of cases [2]. In contrast, right lobe agenesis is more frequently associated with complete isthmus absence. Additionally, a well-documented female predominance exists, though the mechanisms contributing to this gender disparity remain unclear [3].
The pathogenesis of TH likely results from disruptions in key developmental processes, including defective migration, differentiation, or proliferation of thyroid precursor cells. Normal thyroid development begins in the fourth gestational week as an endodermal outpouching from the pharyngeal floor, which elongates into a bilobed structure and descends to its final position in the neck [3]. Any disturbance in this sequence can lead to congenital thyroid anomalies, with TH being one of the rarer manifestations. TH remains underreported due to its typically asymptomatic nature compared to more commonly recognized thyroid malformations, such as thyroglossal duct cysts or ectopic thyroid tissue. This underscores the need for systematic studies to assess its true prevalence and clinical significance [4].
The precise molecular mechanisms underlying TH remain to be understood completely, though evidence suggests a multifactorial etiology involving genetic and environmental influences. Genetic analyses of thyroid dysgenesis have identified key regulatory genes, FOXE1, PAX8, NKX2-1, NKX2-5, and TSHR, which play crucial roles in thyroid organogenesis [3]. While TH is primarily considered a sporadic anomaly, familial clustering, in some cases, suggests the possibility of heritable genetic influences. However, establishing definitive genotype-phenotype correlations remains challenging, as many cases occur in isolation without clear inheritance patterns. The interplay between genetic susceptibility and developmental signaling pathways continues to be an area of ongoing research [5].
Although numerous case reports exist, large-scale case series on TH remain scarce. The rarity of the condition, coupled with its typically benign and asymptomatic presentation, has contributed to a gap in comprehensive epidemiological and developmental studies. This study aims to review a single-center experience in diagnosing and managing TH cases. Additionally, all referenced sources have undergone verification [6].
Methods
Study design and Setting
This study was conducted as a single-center case series at the Thyroid Clinic of Smart Health Tower. The study period extended from July 2021 to July 2024, during which all eligible patients diagnosed with TH were identified and analyzed. The clinic serves as a specialized referral center for thyroid disorders, ensuring comprehensive diagnostic evaluation and follow-up of affected individuals.
Participant Selection and Eligibility Criteria
The study included all patients with a confirmed diagnosis of TH based on ultrasonographic imaging. Patients were eligible for inclusion if they had complete medical records detailing their demographic characteristics, clinical presentation, and radiological findings. Cases with incomplete data, particularly those lacking essential imaging reports or follow-up details, were excluded to ensure consistency and reliability in the analysis.
Data Collection and Variables Assessed
Patient data were systematically retrieved from the hospital’s electronic medical records, radiology reports, and clinicaldocumentation. The collected variables included demographic characteristics such as age, sex, residency, and clinical presentation, including symptoms at diagnosis and the presence of thyroid dysfunction or associated comorbidities. Medical and surgical history, including prior thyroid conditions and interventions, was also documented. Radiological findings focused on the laterality of TH, the size of the contralateral lobe, and any evidence of compensatory hypertrophy. Additionally, laboratory investigations, including thyroid function tests (thyroid stimulating hormone (TSH), triiodothyronine (T3), and thyroxine (T4) levels), were analyzed to assess thyroid function status. Follow-up data were reviewed to evaluate disease progression, changes in thyroid function, and any medical or surgical interventions undertaken.
Data Processing and Statistical Analysis
All collected data were documented and organized using Microsoft Excel 2021. Statistical analyses were conducted using the Statistical Package for the Social Sciences (SPSS) version 27.0. Descriptive statistical methods were employed to summarize the findings, with continuous variables presented as mean and range, while categorical variables were expressed as frequencies and percentages.
Results
This study included 11 patients diagnosed with TH, with a mean age of 28.12 ± 18.14 years (range: <1 to 55 years). The cohort comprised seven females (63.6%) and four males (36.4%). Clinically, six patients (54.5%) were diagnosed incidentally, three (27.3%) presented with neck swelling, and two (18.2%) reported neck pain. Regarding associated congenital conditions, eight patients (72.7%) had no additional anomalies. Among the remaining three, one had a thyroglossal duct cyst, one had a history of prolonged neonatal jaundice, and another presented with both prolonged neonatal jaundice and a periumbilical hernia.
Thyroid function assessment revealed that the majority (7 cases ,63.6%) of patients were euthyroid (0.35-4.5µIU/mL), while two patients exhibited hyperthyroidism (<0.35 µIU/mL), and two of them had hypothyroidism (>4.5 µIU/mL). Ultrasound findings demonstrated left lobe and isthmus agenesis in eight cases (72.7%), while two cases (18.2%) exhibited isolated left lobe agenesis, and one patient exhibited isolated right lobe agenesis (9.1%) (Figures 1 and 2). The largest documented normal lobe measured 100 × 43 × 35 mm, whereas the smallest measured 15 × 6.9 × 7.9 mm. The follow-up period ranged from 4 to 48 months (Tables 1-3).
|
Cases |
Age (Y) |
Gender |
History |
Clinical Thyroid Examinations
|
|||||
|
Presentation |
Duration (W) |
Other Congenital Conditions |
PMH |
PSH |
Drug Hx |
||||
|
Case 1 |
20 |
M |
Neck Swelling |
4 |
None |
Hyperthyroidism |
Negative |
Methimazole |
G2 |
|
Case 2 |
21 |
F |
Neck Pain |
3 |
None |
Negative |
Lymph Node Biopsy |
None |
G2 |
|
Case 3 |
16 |
F |
Incidental |
8 |
Jaundice, Periumbilical Hernia |
Iron Deficiency Anaemia |
Hernia Surgery |
None |
G0 |
|
Case 4 |
<1 |
M |
Incidental |
N/A |
Jaundice |
Hypothyroidism |
Negative |
Thyroxine |
G1 |
|
Case 5 |
31 |
M |
Incidental |
N/A |
None |
Negative |
Negative |
None |
G0 |
|
Case 6 |
55 |
F |
Neck Pain |
8 |
None |
Negative |
Bilateral Total Knee Replacement |
None |
G0 |
|
Case 7 |
26 |
F |
Neck Swelling |
1 |
None |
Negative |
Tonsillectomy |
None |
G2 |
|
Case 8 |
6 |
F |
Neck Swelling |
1 |
Thyroglossal Duct Cyst |
Negative |
Tonsillectomy |
None |
G2 |
|
Case 9 |
55 |
F |
Incidental |
N/A |
None |
Negative |
C-section |
None |
G0 |
|
Case 10 |
53 |
F |
Incidental |
1 |
None |
Negative |
C-section |
None |
G0 |
|
Case 11 |
27 |
M |
Incidental |
3 |
None |
Negative |
Negative |
None |
G0 |
|
M: Male, F: Female, PMH: Past Medical History, PSH: Past Surgical History, Drug Hx: Drug History, G: grades of thyroid enlargement, Y: Years, W: Weeks. |
|||||||||
|
Cases |
Blood Investigations |
Ultrasound Reports |
Follow up (Months) |
|||||
|
First TSH (µIU/mL) |
First Free T4 (pmol/L) |
First Total T4 (nmol/mL) |
ATPO (IU/mL) |
First TRAB (IU/mL) |
Agenesis Side |
Normal Lobe Size (mm) |
||
|
Case 1 |
0.005 |
55.53 |
N/A |
N/A |
12.55 |
Left Lobe, Isthmus |
70 × 26 × 24 |
48 |
|
Case 2 |
2.45 |
19.9 |
N/A |
9 |
N/A |
Left Lobe, Isthmus |
56 × 19 × 19 |
12 |
|
Case 3 |
1.8 |
N/A |
165.6 |
N/A |
N/A |
Left Lobe, Isthmus |
53 × 16 × 14 |
12 |
|
Case 4 |
100 |
2.34 |
N/A |
N/A |
N/A |
Left Lobe |
15 × 6.9 × 7.9 |
8 |
|
Case 5 |
2.61 |
18.00 |
N/A |
68.3 |
N/A |
Left Lobe, Isthmus |
100 × 43 × 35 |
12 |
|
Case 6 |
1.83 |
15.86 |
N/A |
109.2 |
N/A |
Left Lobe, Isthmus |
64 × 31 × 27 |
4 |
|
Case 7 |
1.27 |
16.3 |
N/A |
80.9 |
N/A |
Left Lobe, Isthmus |
55 × 19 × 19 |
6 |
|
Case 8 |
1.33 |
21.71 |
N/A |
N/A |
N/A |
Left Lobe, Isthmus |
34 × 10 × 13 |
36 |
|
Case 9 |
2.27 |
17.02 |
N/A |
11.45 |
N/A |
Left Lobe |
48 × 16 × 15 |
48 |
|
Case 10 |
5.66 |
9.75 |
N/A |
17.6 |
N/A |
Left Lobe, Isthmus |
48 × 18 × 20 |
4 |
|
Case 11 |
0.005 |
41.6 |
9.75 |
N/A |
0.8 |
Right Lobe |
58 × 26 × 25 |
24 |
|
TSH: Thyroid-Stimulating Hormone, T4: Thyroxine, ATPO: Anti-Thyroid Peroxidase Antibodies, TRAB: Thyrotropin Receptor Antibodies, N/A: Not Applicable |
||||||||
|
Variables |
Frequency (percentage) |
|
Gender Male Female |
4 (36.4%) 7 (63.6%) |
|
Age, Years (Mean ± SD) |
28.12 ± 18.14 |
|
Clinical presentations Incidental Neck Pain Neck Swelling |
6 (54.5%) 2 (18.2%) 3 (27.3%) |
|
Past medical history Iron Deficiency Anemia Negative |
1 (9.1%) 10 (90.9%) |
|
Clinical thyroid examination G0 G1 G2 |
6 (54.5%) 1 (9.1%) 4 (36.4%) |
|
Thyroid function status Euthyroid Hyperthyroidism Hypothyroidism |
7 (63.6%) 2 (18.2%) 2 (18.2%) |
|
Agenesis Side Right Left |
1 (9.1%) 10 (90.9%) |
Discussion
The clinical presentation of TH is predominantly asymptomatic, with most cases identified incidentally during imaging studies performed for unrelated thyroid conditions or neck abnormalities. When symptomatic, manifestations typically arise from concurrent thyroid disorders rather than the hemiagenesis itself. These may include neck swelling due to compensatory hypertrophy of the remaining lobe, thyroid dysfunction, or palpable nodules. The prevalence of thyroid abnormalities in individuals with TH appears to increase with age, likely due to chronic overstimulation of the remaining lobe by TSH, a factor contributing to the ongoing debate regarding the benign nature of the condition [7].
In a study in which 40 patients newly diagnosed with TH, aged between 12 and 79, were enrolled, it was found that 90% of their cohort were clinically asymptomatic regarding hemiagenesis itself, with associated conditions including euthyroid nodular goiters, multinodular goiters, Graves’ disease, and Hashimoto’s thyroiditis [8]. Another study emphasized that even symptomatic cases typically arise from coexisting thyroid pathologies rather than the anatomical defect itself [3]. Rare presentations such as hypothyroidism with prolonged neonatal jaundice and umbilical hernia have been documented in pediatric cases [3]. In the present study, 54.5% of patients were diagnosed incidentally, a lower rate than previously reported in the literature. A notable proportion exhibited clinical symptoms, with neck swelling in 27.3% and neck pain in 18.2% of cases, suggesting potential variations in clinical presentation, particularly among younger populations. Furthermore, congenital anomalies, including thyroglossal duct cyst, prolonged neonatal jaundice, and periumbilical hernia, were observed in 27.3% of cases, findings not prominently reported in earlier studies. These variations highlight the need for further investigation into potential demographic and pathophysiological factors influencing the clinical spectrum of TH.
The diagnosis of TH is mainly based on imaging modalities, with ultrasonography as the first-line investigation and thyroid scintigraphy as a complementary confirmatory tool. Ultrasound imaging is particularly valuable as the initial screening method due to its wide availability, lack of radiation exposure, and sensitivity in detecting the absence of a thyroid lobe and any structural changes in the remaining thyroid tissue [3]. Thyroid scintigraphy using technetium or iodine provides functional anatomical assessment with the advantage of detecting ectopic thyroid tissue and diagnosing concurrent thyroid pathologies in the remaining lobe. Combining these two imaging modalities remains essential for accurate diagnosis and differentiation from other conditions that might mimic hemiagenesis [3]. A large cohort case-control study by Ruchala et al. emphasizes the need for both ultrasonography and scintigraphy to distinguish true hemiagenesis from pseudoagenesis, which can occur in cases of severe atrophy or destruction of thyroid tissue [8]. In a study focused on pediatric cases with suspected thyroid dysgenesis, researchers utilized both thyroid scanning and ultrasonography to establish definitive diagnoses, with hemiagenesis identified in one of their subjects [9]. Another case report of a rare male pediatric patient with TH demonstrated how ultrasonography revealed the absence of the left lobe while the right lobe showed minimal hyperplasia without nodules; scintigraphy confirmed these findings and ruled out ectopic thyroid tissue. This case emphasized that when only one thyroid lobe is detected initially, physicians should consider TH and employ both imaging modalities before invasive procedures [10].
A retrospective evaluation of imaging for congenital hypothyroidism revealed that compared to 99mTc-pertechnetate scanning, ultrasound examination demonstrated 100% specificity but only 44% sensitivity for detecting thyroid abnormalities. This finding highlights the value of scintigraphy as a complementary method to ultrasound examination, particularly when ectopic thyroid tissue is suspected. The limitations of relying solely on ultrasonography were further illustrated in cases where thyroid agenesis was diagnosed with ultrasonography, but follow-up scintigraphy revealed sublingual thyroid tissue in a significant proportion of patients [11]. In the current study, ultrasonography was the primary diagnostic tool, revealing left lobe and isthmus agenesis in eight (72.7%) cases, while two cases (18.2%) exhibited isolated left lobe agenesis with preservation of the isthmus, and one case showed isolated right lobe agenesis with preserved isthmus (9.1%). The ultrasound findings documented normal lobe dimensions ranging from the smallest at 15 × 6.9 × 7.9 mm to the largest at 100 × 43 × 35 mm, providing valuable reference values for assessing potential compensatory hypertrophy.
Typically, TH is associated with normal thyroid function, as the remaining lobe compensates for the absent tissue. Most patients remain euthyroid, though biochemical patterns may reveal elevated TSH levels despite normal peripheral hormone concentrations, suggesting mild subclinical hypothyroidism or compensatory stimulation of the intact lobe. Functional thyroid disorders such as hyperthyroidism or hypothyroidism may coexist, often linked to concurrent pathologies like autoimmune thyroiditis or nodular goiter [3,12]. Recent studies highlight these trends. Ruchała et al. noted that while TSH and free T3 levels were elevated in TH patients compared to controls, most maintained euthyroidism [8]. Maiorana et al. documented subclinical hypothyroidism in pediatric cases [13]. Genetic factors, including potential PAX8 or FOXE1 gene involvement, may influence thyroid development but do not directly correlate with hormonal status [14]. Management focuses on addressing associated thyroid disorders rather than the anatomical defect itself. For asymptomatic patients, periodic monitoring with ultrasonography and thyroid function tests suffices [3,12]. Surgical intervention is indicated for malignancies or symptomatic nodules in the remaining lobe, necessitating lifelong thyroxine supplementation post-resection [14]. The current study aligns with these findings since 63.6% of patients were euthyroid, and only two cases of hyperthyroidism and two of hypothyroidism were identified, each requiring specific targeted therapy. While compensatory hypertrophy was observed, no evidence of progressive dysfunction emerged during follow-up, reinforcing the conservative approach for uncomplicated TH [3].
The follow-up and outcome of TH primarily focus on monitoring for potential thyroid pathologies and ensuring optimal thyroid function. Since TH itself is generally asymptomatic, the clinical significance lies in its association with other thyroid disorders. Therefore, regular follow-ups with thyroid function tests and ultrasonography are crucial to detect emerging thyroid conditions early. Recent studies emphasize the importance of long-term monitoring. For instance, a study by Peteiro-Gonzalez et al. highlighted that patients with TH are more prone to autoimmune thyroid disease and nodular goiter due to sustained compensatory stimulation of the remaining lobe, necessitating regular surveillance to manage these conditions effectively [12]. Another study suggested that patients with TH might benefit from thyroxine therapy to normalize TSH levels and potentially prevent associated thyroid pathologies. However, further research is needed to confirm this approach. In cases where TH coexists with malignancies like medullary thyroid cancer, follow-up involves regular biochemical monitoring (calcitonin and carcinoembryonic antigen levels) and ultrasonography to detect recurrence early [15]. The current study's follow-up period ranged from 4 to 48 months, with no significant thyroid dysfunction or complications reported during this time. The study's findings align with previous literature in emphasizing the need for ongoing surveillance to manage potential thyroid-related issues in patients with TH. Despite the absence of severe complications during the study period, the importance of continued monitoring cannot be overstated, given the potential for future development of thyroid pathologies in these patients.
One of the primary limitations of this study is the unavailability of advanced diagnostic tools such as thyroid scintigraphy and molecular genetic testing. Scintigraphy, which is considered the complementary tool for confirming thyroid hemiagenesis, was not performed in any of the cases due to lack of access to nuclear medicine facilities. However, all cases were assessed using high-resolution ultrasonography performed by experienced clinicians in a high-volume, thyroid-specialized center, supporting the reliability of the diagnoses. Similarly, molecular or genetic analyses that could provide insights into potential hereditary or developmental mechanisms were not feasible, primarily due to financial constraints and limited infrastructure in the setting of a developing country.
Conclusion
This study confirms the female predominance of TH, with a higher prevalence of left-lobe absence and frequent symptomatic presentations. The association with congenital anomalies suggests embryological links requiring further exploration. While thyroid function is generally preserved, cases of hypo- and hyperthyroidism underscore the need for individualized endocrine evaluation.
Declarations
Conflicts of interest: The authors have no conflicts of interest to disclose.
Ethical approval: Ethical approval for this study was obtained from the Ethics Committee of the Kscien Organization (Approval No. 2025-37)
Consent for participation: Not applicable.
Consent for publication: Written informed consent for publication was obtained from the patients or, in the case of minors, from their parents.
Funding: The present study received no financial support.
Acknowledgements: None to be declared.
Authors' contributions: AMS, HOB, ShFA, and AMM: Major contributors to the conception of the study, as well as the literature search for related studies, and manuscript writing. KMS, AQQ, SHH, HAA, AJQ and ROM: Literature review, design of the study, critical revision of the manuscript, and processing of the tables. ANQ, AHA, DHH, and RRR: Literature review, processing of the figures, data analysis and interpretation.
Use of AI: ChatGPT-3.5 was used to assist with language refinement and improve the overall clarity of the manuscript. All content was thoroughly reviewed and approved by the authors, who bear full responsibility for the final version.
Data availability statement: Not applicable.
Systematic Review and Meta-analyses
Current Perspectives on Cystic Echinococcosis: A Systematic Review
Hawkar A. Nasralla, Berun A. Abdalla, Hiwa O. Abdullah, Sasan M. Ahmed, Fahmi H. Kakamad, Shvan...
Abstract
Introduction: Hydatidosis, a zoonotic disease caused by the larval stage of Echinococcus granulosus, is a significant public health concern with notable economic impact. It leads to morbidity and mortality worldwide, particularly in endemic regions. This study systematically reviews recent literature on cystic echinococcosis (CE) to provide updated insights into its prevalence, impact, and management.
Methods: A systematic review was conducted using PubMed to find original articles on hydatid cysts published between
September 1, 2019, and September 1, 2024. Data extracted included the first author's name, country, publication year, study type, number of cases, clinical presentation, diagnostic methods, cyst location and quantity, cyst status, treatment type and medications, follow-up details, recurrence, and mortality rates. Data were organized and qualitatively analyzed.
Results: A total of 398 articles were identified, of which 229 articles with 1,002 patients met the inclusion criteria. Spain reported the highest number of CE cases at 362 (36.13%). Asia accounted for 487 cases (48.60%), and Europe contributed 460 cases (45.91%). The liver was the most frequently affected organ, accounting for 731 cases (72.95%), followed by the lungs with 110 cases (10.98%), and the kidney with 43 cases (4.29%). The age distribution of the cases showed that 63 (6.29%) were aged between 3 and 18 years.
Conclusion: Hydatidosis remains a significant global public health concern, impacting developing and developed countries. The liver and lungs remain the primary sites of infection. Preventive strategies, including regular animal screening and enhanced public health education, are essential for controlling the spread of the disease.
Introduction
Cystic echinococcosis (CE), also known as hydatid disease (HD) or hydatidosis, is a well-known zoonotic disease caused by the larval stage of the tapeworm Echinococcus granulosus. Humans usually act as intermediate hosts, contracting the infection through direct contact with primary hosts like sheep, goats, cattle, dogs, and other canines or consuming food and water contaminated with the parasite's eggs [1, 2].
To date, HD is a serious public health problem that carries considerable economic implications. It leads to morbidity and mortality in various regions, notably in Mediterranean countries, the Middle East, New Zealand, Australia, India, and South America, mainly due to the close connections between sheep, dogs, and humans. It remains a neglected disease in many regions, necessitating concerted efforts for prevention and control, especially in rural areas where it is more prevalent [3, 4].
Hydatidosis can affect nearly any part of the body, but the liver is the organ most frequently impacted (75%), followed by the lungs (15%) and other organs like the brain (2%) and spine (1%) [3]. Hydatidosis is marked by a prolonged asymptomatic incubation period, often lasting several years. Clinical symptoms appear when the cysts grow large enough to compress nearby tissues. Additionally, cyst rupture into the peritoneal cavity can result in secondary cyst formation and the development of daughter cysts within them [3, 4]. This study systematically reviews recent literature on CE to provide updated insights into its prevalence, impact, and management.
Methods
Study design
This systematic review was conducted according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines.
Data sources and search strategy
A systematic review was performed using PubMed to identify original articles on hydatid cysts. The search strategy targeted recent, peer-reviewed clinical studies on echinococcosis in human populations, published from September 1, 2019, to September 1, 2024, and restricted to English-language research. The search was limited to the literature of the last five years to shed light on the current disease situation.
Eligibility criteria
This systematic review included only original studies and case reports. Exclusion criteria were as follows: 1) articles not in English, 2) abstract only, 3) studies on alveolar echinococcosis, 4) studies unrelated to humans, 5) inadequately peer-reviewed articles, and 6) any study types that did not meet the inclusion criteria. All references in this study were evaluated for eligibility [5].
Study selection and data extraction
The titles and abstracts of the selected studies were initially screened, followed by an in-depth full-text review to assess eligibility. Data extracted from each included study encompassed the first author’s name, country of origin, publication year, study type, number of cases, clinical presentation, diagnostic approaches, hydatid cyst location, cyst quantity, cyst status (intact or ruptured), treatment type, medications used, follow-up details, recurrence rate, and mortality rate.
Statistical analyses
Data were organized in an Excel spreadsheet (Microsoft Excel, 2021) and qualitatively analyzed using the Statistical Package for the Social Sciences (SPSS, version 27.0). Key findings were summarized as median, range, frequencies, and percentages.
Results
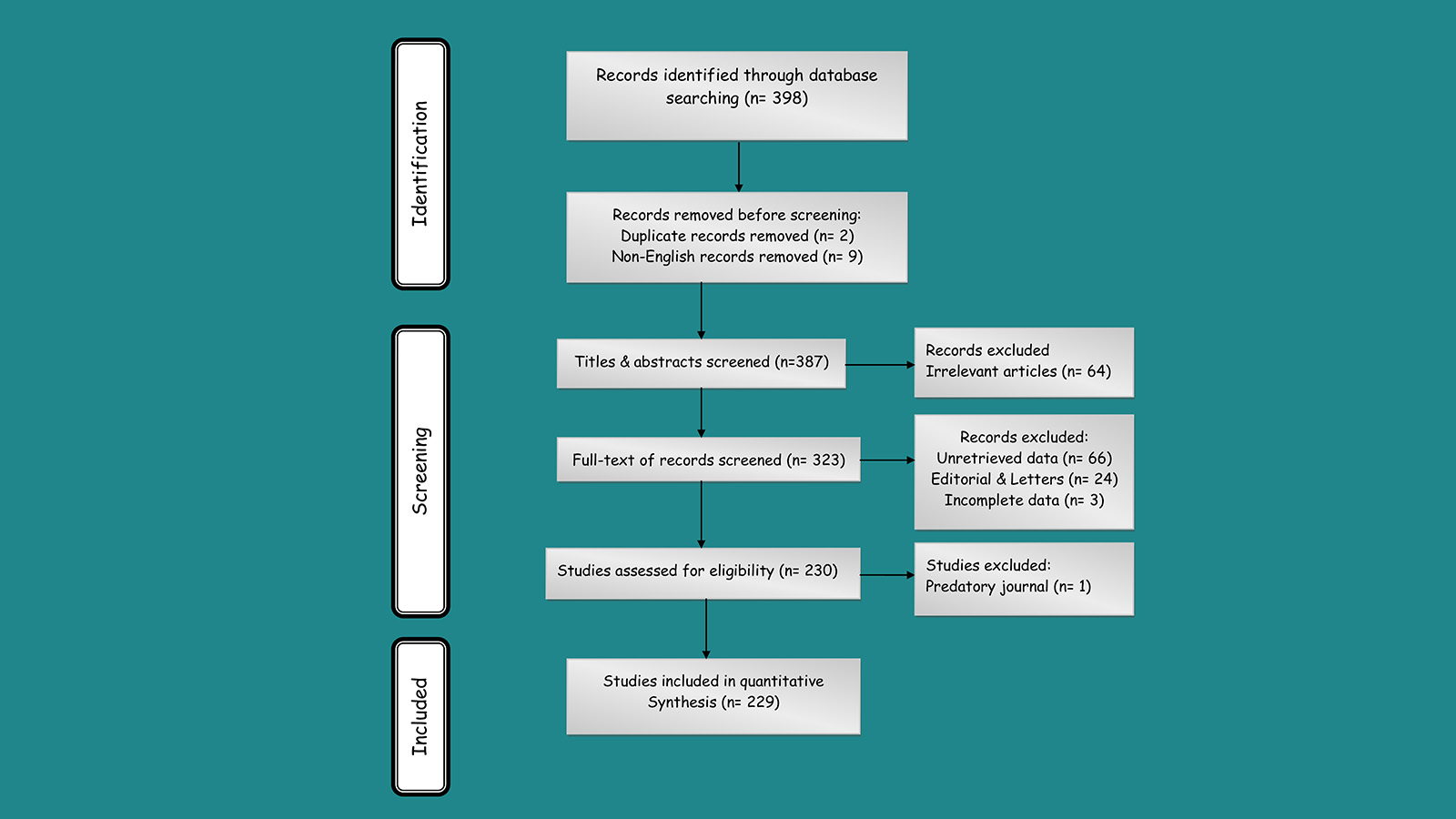
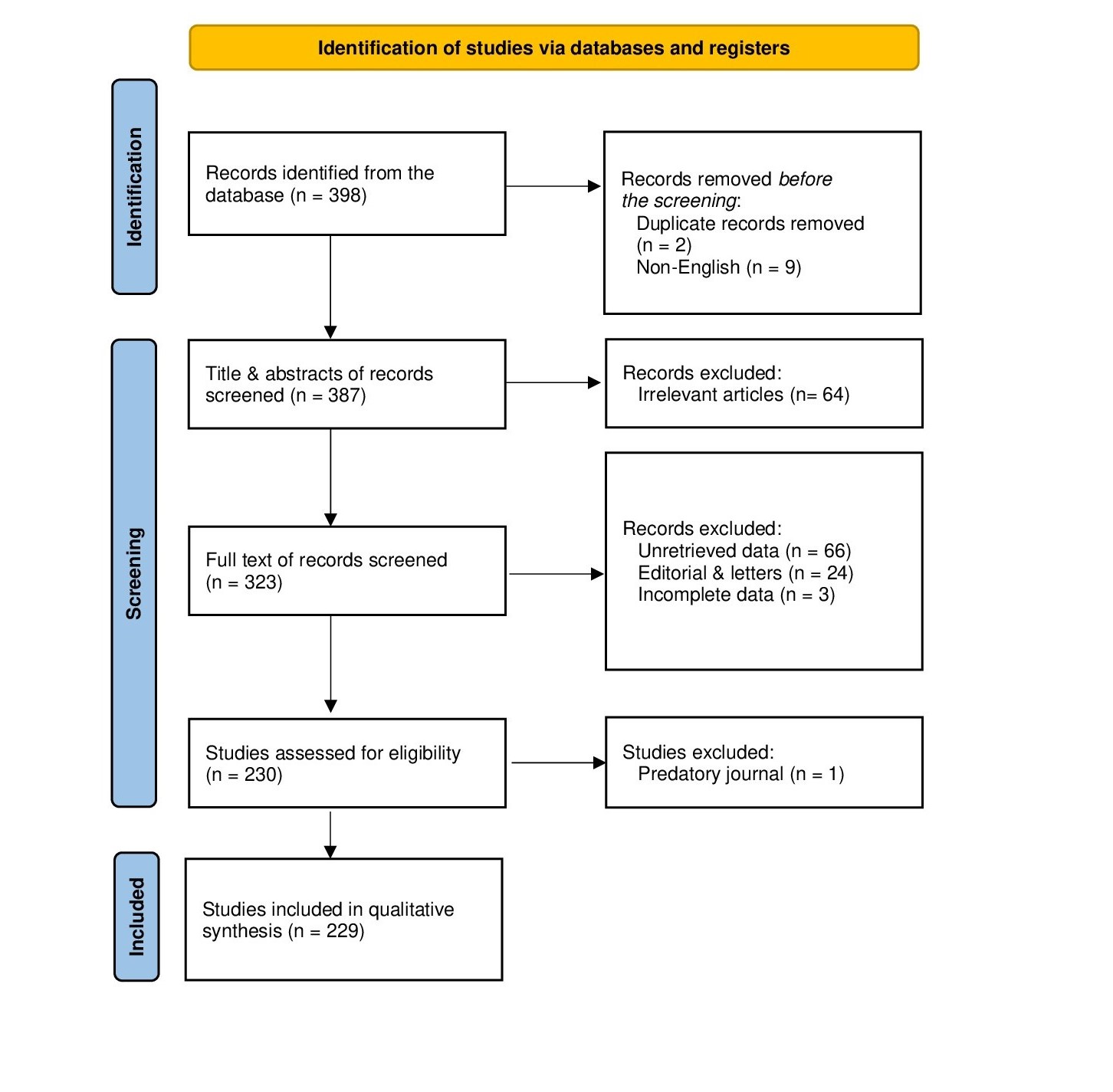
A total of 398 articles were identified through the search. After an initial review, 11 articles were excluded due to duplication and non-English language. The remaining 387 articles underwent title and abstract screening, during which 64 articles were excluded for not meeting the inclusion criteria. Consequently, 323 articles proceeded to full-text screening, and 93 were excluded due to unretrievable data, editorials, letters, or incomplete information. The remaining articles were then assessed for eligibility, resulting in 229 articles [1, 3, 4, 6-231] with 1,002 patients meeting the inclusion criteria and included in the study [Fig. 1].
Among the included studies, 217 (94.76%) were case reports, seven (3.06%) were cohort studies, three (1.31%) were case series, one (0.44%) was a cross-sectional study, and one (0.44%) was a randomized controlled trial (Table 1). Among the countries, Spain recorded the highest number of cases with 362 (36.13%), followed by China with 270 cases (26.95%) and Turkey with 128 cases (12.77%), collectively accounting for approximately 75% of the total reported cases (Table 2). In terms of continental distribution, Asia recorded 487 cases (48.60%), while Europe was not far behind with 460 cases (45.91%) (Table 3).
|
First Author, Year |
Study design |
Country |
No. of cases |
First Author, Year |
Study design |
Country |
No. of cases |
First Author, Year |
Study design |
Country |
No. of cases |
|
AlRashed, 2024 [1] |
A |
Saudi Arabia |
1 |
Mutlu, 2022 [82] |
A |
Turkey |
1 |
Gatt, 2020 [157] |
A |
Israel |
1 |
|
Amer, 2024 [6] |
A |
Iran |
1 |
Ozgokce, 2022 [83] |
A |
Turkey |
1 |
Giri, 2020 [158] |
A |
Bhutan |
1 |
|
Babiker, 2024 [7] |
A |
Qatar |
1 |
Passarelli, 2022 [84] |
A |
US |
1 |
Gopivallabha, 2020 [159] |
A |
India |
1 |
|
Bazzi, 2024 [8] |
A |
Lebanon |
1 |
Pulavarty, 2022 [85] |
A |
India |
1 |
Delgado, 2020 [160] |
A |
Spain |
1 |
|
Brezeanu, 2024 [9] |
A |
Romania |
1 |
Rodríguez-Laiz, 2022 [86] |
A |
Spain |
1 |
Handran, 2020 [161] |
A |
US |
1 |
|
Calu, 2024 [10] |
A |
Romania |
2 |
Sezer, 2022 [87] |
A |
Turkey |
1 |
İriz, 2020 [162] |
A |
Turkey |
1 |
|
Chen, 2024 [11] |
A |
Taiwan |
1 |
Shahid, 2022 [88] |
A |
Pakistan |
1 |
İyigün, 2020 [163] |
A |
Turkey |
1 |
|
Darestani, 2024 [12] |
A |
Iran |
1 |
Sharma, 2022 [89] |
A |
India |
1 |
Jarovsky, 2020 [164] |
A |
Brazil |
1 |
|
Ghaedamini, 2024 [13] |
A |
Iran |
1 |
Sozutok, 2022 [90] |
A |
Turkey |
1 |
Johny, 2020 [165] |
A |
India |
1 |
|
Gulati, 2024 [14] |
A |
US |
1 |
Sun, 2022 [91] |
B |
China |
2 |
Kankilic, 2020 [166] |
B |
Turkey |
6 |
|
Hasnaoui, 2024 [15] |
A |
Tunisia |
1 |
Ulusoy, 2022 [92] |
A |
Turkey |
1 |
Kaskar, 2020 [167] |
A |
India |
1 |
|
Haydar, 2024 [16] |
A |
Iran |
1 |
Uzunoğlu, 2022 [93] |
A |
Turkey |
1 |
Kiran, 2020 [168] |
A |
India |
1 |
|
Jalayeri, 2024 [17] |
A |
Iran |
1 |
Wang, 2022 [94] |
A |
China |
1 |
Kırmacı, 2020 [169] |
A |
Turkey |
1 |
|
Jellali, 2024 [18] |
A |
Tunisia |
1 |
Agarwal, 2021 [95] |
A |
India |
1 |
Kumar, 2020 [170] |
A |
India |
1 |
|
Karahan, 2024 [19] |
A |
India |
1 |
Aghajanzadeh, 2021 [4] |
A |
Iran |
1 |
Lahdhil, 2020 [171] |
A |
Tunisia |
1 |
|
Koren, 2024 [20] |
A |
Israel |
1 |
Aili, 2021 [96] |
A |
China |
1 |
Lapierre, 2020 [172] |
A |
Canada |
1 |
|
Mahesan, 2024 [21] |
A |
India |
1 |
Akhan, 2021 [97] |
A |
Turkey |
1 |
Llanos, 2020 [173] |
A |
US |
1 |
|
Bouhout, 2024 [22] |
A |
Morocco |
1 |
Basne, 2021 [98] |
A |
Nepal |
1 |
Lodhia, 2020 [174] |
A |
Tanzania |
2 |
|
Manuel, 2024 [23] |
A |
Angola |
1 |
Biswas, 2021 [99] |
A |
India |
3 |
Lyske, 2020 [175] |
A |
Canada |
1 |
|
Mierzejewski, 2024 [24] |
A |
Poland |
1 |
Boumarah, 2021 [100] |
A |
Saudi Arabia |
1 |
Ma, 2020 [176] |
E |
China |
195 |
|
Mutlu, 2024 [25] |
A |
Turkey |
1 |
Çankaya, 2021 [101] |
A |
Turkey |
1 |
Mitrovic, 2020 [177] |
A |
Serbia |
1 |
|
Remmerswaal, 2024 [26] |
A |
Netherlands |
1 |
Cathomas, 2021 [102] |
A |
Switzerland |
2 |
Mittal, 2020 [178] |
A |
India |
1 |
|
Reyimu, 2024 [27] |
A |
China |
1 |
Chatzifotiou, 2021 [103] |
A |
Germany |
1 |
Moghtadaie, 2020 [179] |
A |
Iran |
1 |
|
Sączek, 2024 [28] |
A |
Poland |
1 |
Christodouli dis, 2021 [3] |
C |
Greece |
50 |
Nistor, 2020 [180] |
A |
Romania |
1 |
|
Thakar, 2023 [29] |
A |
India |
1 |
Ciftci, 2021 [104] |
C |
Turkey |
34 |
Ogul, 2020 [181] |
A |
Turkey |
1 |
|
Voicu, 2024 [30] |
A |
Romania |
1 |
Conlon, 2021 [105] |
A |
Ireland |
1 |
Pappas, 2020 [182] |
A |
Greece |
1 |
|
Aarif, 2023 [31] |
A |
India |
1 |
Elvan-Tuz, 2021 [106] |
A |
Turkey |
2 |
Ramia, 2020 [183] |
C |
Spain |
71 |
|
Alsulami, 2023 [32] |
A |
Saudi Arabia |
1 |
Gautam, 2021 [107] |
A |
India |
1 |
Samadian, 2020 [184] |
A |
Iran |
1 |
|
Ammar, 2023 [33] |
A |
Tunisia |
1 |
Ghabisha, 2021 [108] |
A |
Yemen |
1 |
Sangal, 2020 [185] |
A |
India |
1 |
|
Borni, 2023 [34] |
A |
Tunisia |
1 |
Gonder, 2021 [109] |
C |
Turkey |
9 |
Sauteur, 2020 [186] |
A |
Switzerland |
1 |
|
Carrel, 2023 [35] |
A |
Uzbekistan |
1 |
Govindaraj, 2021 [110] |
A |
India |
1 |
Savu, 2020 [187] |
A |
Romania |
1 |
|
Casulli, 2023 [36] |
A |
Italy |
1 |
Guha, 2021 [111] |
A |
India |
1 |
Schleenvoigt, 2020 [188] |
A |
Germany |
1 |
|
Caushi, 2023 [37] |
A |
Albania |
1 |
Hãlmaciu, 2021 [112] |
A |
Romania |
1 |
Singh, 2020 [189] |
A |
India |
1 |
|
Das, 2023 [38] |
A |
India |
1 |
Harmouchi, 2021 [113] |
A |
Morocco |
1 |
Singh, 2020 [190] |
A |
India |
1 |
|
Galvis, 2023 [39] |
A |
Colombia |
1 |
Helvaci, 2021 [114] |
A |
Turkey |
1 |
Singla, 2020 [191] |
A |
India |
1 |
|
Göktürk, 2023 [40] |
A |
Turkey |
1 |
Hermosa, 2021 [115] |
A |
Spain |
1 |
Sonsoz, 2020 [192] |
A |
Turkey |
1 |
|
Hakimi, 2023 [41] |
A |
Afghanistan |
1 |
Iken, 2021 [116] |
A |
Morocco |
1 |
Tekin, 2020 [193] |
A |
Turkey |
1 |
|
Hasnaoui, 2023 [42] |
A |
Tunisia |
1 |
Jaén-Torrejimeno, 2021 [117] |
C |
Spain |
287 |
Tlili, 2020 [194] |
A |
Tunisia |
1 |
|
Jia, 2023 [43] |
A |
China |
1 |
Jindal, 2021 [118] |
A |
India |
1 |
Tonkaz, 2020 [195] |
A |
Turkey |
1 |
|
Kardoun, 2023 [44] |
A |
Tunisia |
1 |
Kafadar, 2021 [119] |
A |
Turkey |
1 |
Van De, 2020 [196] |
A |
Korea |
2 |
|
Lao, 2023 [45] |
A |
China |
1 |
Kankam, 2021 [120] |
A |
Iran |
1 |
Vasilescu, 2020 [197] |
A |
Romania |
1 |
|
Lees, 203 [46] |
A |
UK |
1 |
Kechiche, 2021 [121] |
B |
Tunisia |
10 |
Verma, 2020 [198] |
A |
India |
1 |
|
Li, 2023 [47] |
A |
China |
1 |
Khasawneh, 2021 [122] |
A |
Jordan |
2 |
Villalobos, 2020 [199] |
A |
US |
1 |
|
Ma, 2023 [48] |
A |
China |
1 |
Kumar, 2021 [123] |
A |
India |
1 |
Xu, 2020 [200] |
A |
China |
1 |
|
Maggioni, 2023 [49] |
A |
Italy |
1 |
Li, 2021 [124] |
A |
China |
1 |
Yang, 2020 [201] |
A |
China |
1 |
|
Mahmood, 2023 [50] |
A |
Pakistan |
1 |
Maliqari, 2021 [125] |
A |
Albania |
1 |
Yimamu, 2020 [202] |
A |
China |
1 |
|
Mayekar, 2023 [51] |
A |
India |
1 |
Moshref, 2021 [126] |
A |
Saudi Arabia |
1 |
Abbas, 2019 [203] |
A |
Morocco |
1 |
|
Moraes, 2023 [52] |
A |
Brazil |
1 |
Mozafar, 2021 [127] |
A |
Iran |
1 |
Aydin, 2019 [204] |
A |
Turkey |
1 |
|
Moscatelli, 2023 [53] |
A |
Argentina |
1 |
Rabhi, 2021 [128] |
A |
Tunisia |
1 |
Banerjee, 2019 [205] |
A |
India |
1 |
|
Ntombela, 2023 [54] |
A |
South Africa |
2 |
Rhissassi, 2021 [129] |
A |
Morocco |
1 |
Beyhan, 2019 [206] |
A |
Turkey |
1 |
|
Peralta, 2023 [55] |
A |
Ecuador |
1 |
Safari, 2021 [130] |
A |
Iran |
1 |
Bracha, 2019 [207] |
A |
Israel |
2 |
|
Peulier‐Maitre, 2023 [56] |
A |
France |
1 |
Shakerian, 2021 [131] |
A |
Iran |
1 |
Chaouch, 2019 [208] |
A |
Tunisia |
1 |
|
Ruíz-Pérez, 2023 [57] |
A |
Peru |
1 |
Sharifi, 2021 [132] |
A |
Iran |
1 |
Demir, 2019 [209] |
A |
Turkey |
1 |
|
Safarpour, 2023 [58] |
A |
Iran |
2 |
Sharma, 2021 [133] |
A |
India |
1 |
Derbel, 2019 [210] |
A |
Tunisia |
1 |
|
Shah, 2023 [59] |
A |
India |
1 |
Shuaibi, 2021 [134] |
A |
US |
1 |
Gök, 2019 [211] |
A |
Turkey |
1 |
|
Türkoğlu, 2023 [60] |
A |
Turkey |
1 |
Simsek, 2021 [135] |
A |
Turkey |
3 |
Kandemirli, 2019 [212] |
A |
Turkey |
1 |
|
Wang, 2023 [61] |
A |
China |
1 |
Şimşek, 2021 [136] |
A |
Turkey |
1 |
Kang, 2019 [213] |
A |
Korea |
1 |
|
Ahmady‑Nezhad, 2023 [62] |
A |
Iran |
1 |
Singh, 2021 [137] |
A |
India |
1 |
Kaya, 2019 [214] |
A |
Turkey |
1 |
|
Assefa, 2022 [63] |
A |
Ethiopia |
1 |
Ucar, 2021 [138] |
A |
Turkey |
1 |
Khullar, 2019 [215] |
A |
India |
1 |
|
Bicer, 2022 [64] |
A |
Turkey |
1 |
van Zijl, 2021 [139] |
A |
South Africa |
1 |
Kuzmanovska, 2019 [216] |
A |
Macedonia |
2 |
|
Bishnoi, 2022 [65] |
A |
India |
1 |
Velho, 2021 [140] |
A |
Portugal |
1 |
MadissonBernardo, 2019 [217] |
A |
Brazil |
1 |
|
Castro, 2022 [66] |
A |
Brazil |
1 |
Wang, 2021 [141] |
A |
China |
1 |
Magistri, 2019 [218] |
C |
Italy |
15 |
|
Dantis, 2022 [67] |
A |
India |
1 |
Wu, 2021 [142] |
A |
China |
1 |
Milosavljevic, 2019 [219] |
A |
Serbia |
1 |
|
Dere, 2022 [68] |
A |
Turkey |
1 |
Yasin, 2021 [143] |
A |
Malaysia |
1 |
Ramteke, 2019 [220] |
A |
India |
2 |
|
Fourati, 2022 [69] |
A |
Tunisia |
1 |
Zedelj, 2021 [144] |
A |
Croatia |
1 |
Sharma, 2019 [221] |
A |
India |
1 |
|
González Arboleda, 2022 [70] |
A |
Chile |
1 |
Zhang, 2021 [145] |
A |
China |
1 |
Singh, 2019 [222] |
A |
India |
1 |
|
Hammade, 2022 [71] |
A |
Syria |
1 |
Zouaghi, 2021 [146] |
A |
Tunisia |
1 |
Syllaios, 2019 [223] |
A |
Greece |
1 |
|
Hanalioglu, 2022 [72] |
A |
Turkey |
1 |
Aboksari, 2020 [147] |
A |
Iran |
1 |
Taşlıçay, 2019 [224] |
A |
Turkey |
1 |
|
Çeviker,2022 [73] |
A |
Turkey |
1 |
Acharya, 2020 [148] |
A |
Nepal |
1 |
Tonkaz, 2019 [225] |
A |
Turkey |
1 |
|
Huertas, 2022 [74] |
A |
Spain |
1 |
Akhan, 2020 [149] |
D |
Turkey |
38 |
Trawinski, 2019 [226] |
A |
Germany |
1 |
|
Ijaz, 2022 [75] |
A |
Pakistan |
1 |
Akhtar, 2020 [150] |
A |
India |
1 |
Wa, 2019 [227] |
A |
China |
1 |
|
Karahan, 2022 [76] |
A |
Turkey |
1 |
Arora, 2020 [151] |
A |
India |
1 |
Wang, 2019 [228] |
A |
China |
1 |
|
Karami, 2022 [77] |
A |
Iran |
1 |
Assimakopoulos, 2020 [152] |
A |
Greece |
1 |
Xu, 2019 [229] |
A |
China |
1 |
|
Kartavya, 2022 [78] |
A |
India |
1 |
Bakshi, 2020 [153] |
A |
India |
1 |
Yacine, 2019 [230] |
A |
Tunisia |
1 |
|
Kumar, 2022 [79] |
A |
India |
1 |
Destek, 2020 [154] |
A |
Turkey |
1 |
Zhuoli, 2019 [231] |
A |
China |
1 |
|
Li, 2022 [80] |
C |
China |
53 |
Dkhissi, 2020 [155] |
A |
Morocco |
1 |
||||
|
Li, 2022 [81] |
A |
China |
1 |
Ewnte, 2020 [156] |
A |
Ethiopia |
1 |
||||
|
A: case report, B: case series, C: cohort, D: randomized control trial, E: cross-sectional study, US: United States, UK: United Kingdom |
|||||||||||
|
Country |
Number of Cases |
Percentage (%) |
|
Spain |
362 |
36.13% |
|
China |
270 |
26.95% |
|
Turkey |
128 |
12.77% |
|
Greece |
53 |
5.29% |
|
India |
44 |
4.39% |
|
Tunisia |
24 |
2.40% |
|
Iran |
18 |
1.80% |
|
Italy |
17 |
1.70% |
|
Romania |
8 |
0.80% |
|
Morocco |
6 |
0.60% |
|
United States |
6 |
0.60% |
|
Brazil |
4 |
0.40% |
|
Israel |
4 |
0.40% |
|
Saudi Arabia |
4 |
0.40% |
|
Germany |
3 |
0.30% |
|
Pakistan |
3 |
0.30% |
|
South Africa |
3 |
0.30% |
|
South Korea |
3 |
0.30% |
|
Switzerland |
3 |
0.30% |
|
Albania |
2 |
0.20% |
|
Canada |
2 |
0.20% |
|
Ethiopia |
2 |
0.20% |
|
Jordan |
2 |
0.20% |
|
Macedonia |
2 |
0.20% |
|
Nepal |
2 |
0.20% |
|
Poland |
2 |
0.20% |
|
Serbia |
2 |
0.20% |
|
Tanzania |
2 |
0.20% |
|
Afghanistan |
1 |
0.10% |
|
Angola |
1 |
0.10% |
|
Argentina |
1 |
0.10% |
|
Bhutan |
1 |
0.10% |
|
Chile |
1 |
0.10% |
|
Colombia |
1 |
0.10% |
|
Croatia |
1 |
0.10% |
|
Ecuador |
1 |
0.10% |
|
France |
1 |
0.10% |
|
Ireland |
1 |
0.10% |
|
Lebanon |
1 |
0.10% |
|
Malaysia |
1 |
0.10% |
|
Netherlands |
1 |
0.10% |
|
Peru |
1 |
0.10% |
|
Portugal |
1 |
0.10% |
|
Qatar |
1 |
0.10% |
|
Syria |
1 |
0.10% |
|
Taiwan |
1 |
0.10% |
|
United Kingdom |
1 |
0.10% |
|
Uzbekistan |
1 |
0.10% |
|
Yemen |
1 |
0.10% |
|
Continent |
Number of cases |
Percentage (%) |
|
Asia |
487 |
48.60% |
|
Europe |
460 |
45.91% |
|
Africa |
38 |
3.79% |
|
South America |
9 |
0.90% |
|
North America |
8 |
0.80% |
The liver was the most frequently affected organ, accounting for 731 cases (72.95%), followed by the lungs with 110 cases (10.98%), the kidney with 43 cases (4.29%), the heart with 37 cases (3.69%), and muscle tissue with 24 cases (2.40%) (Table 4). The gender distribution among the cases was nearly equal, with 505 males (50.40%) and 496 females (49.50%). The age distribution revealed that 63 cases (6.29%) were between 3 and 18 years old, while the age of 740 patients (73.85%) was unspecified. Among the identified cases, the median age was 35 (QR:19-51) years. The most common clinical presentations included pain (18.86%), fever (6.59%), shortness of breath (4.09%), and cough (2.69%), with 51 cases (5.09%) being asymptomatic. Clinical presentation was not documented for 616 cases (61.48%). Regarding cyst characteristics, single cysts were identified in 466 cases (46.51%), and intact cysts were found in 100 patients (9.98%). Treatment predominantly involved surgical intervention, performed in 639 cases (63.77%), and Albendazole was the most commonly prescribed medication, given in 275 cases (27.44%). Follow-up data revealed that 347 patients were monitored for less than six months (34.63%). Recurrence was observed in 26 cases (2.59%), and mortality occurred in 17 patients (1.70%) (Table 5).
|
Organ |
Number of cases* |
Percentage (%) |
|
Liver |
731 |
72.95% |
|
Lung |
110 |
10.98% |
|
Kidney |
43 |
4.29% |
|
Heart |
37 |
3.69% |
|
Muscle |
24 |
2.40% |
|
Brain |
21 |
2.10% |
|
Abdominal cavity |
16 |
1.60% |
|
Bone |
14 |
1.40% |
|
Vertebral and spinal region |
14 |
1.40% |
|
Pelvic region |
12 |
1.20% |
|
Pancreas |
9 |
0.90% |
|
Spleen |
8 |
0.80% |
|
Mediastinum |
5 |
0.50% |
|
Breast |
4 |
0.40% |
|
Uterus |
4 |
0.40% |
|
Intra-orbital |
3 |
0.30% |
|
Thyroid gland |
2 |
0.20% |
|
Gallbladder |
1 |
0.10% |
|
Others |
14 |
1.40% |
|
* Some patients had hydatid cysts in more than one organ. |
||
|
Variables |
Frequency (percentage) |
|
Gender Male Female Non-Identified |
505 (50.40%) 496 (49.50%) 1 (0.10%) |
|
Age (year) 3 – 18 19 – 30 31 – 40 41 – 50 51 – 60 61 – 70 > 70 N/A Median (QR) |
63 (6.29%) 52 (5.19%) 47 (4.69%) 34 (3.39) 18 (1.80%) 28 (2.79%) 20 (2.00%) 740 (73.85%) 35 (19–51) |
|
Clinical presentations* Pain Fever Shortness of breath Cough Asymptomatic Others N/A |
189 (18.86%) 66 (6.59%) 41 (4.09%) 27 (2.69%) 51 (5.09%) 42 (4.19%) 616 (61.48%) |
|
Diagnostic findings |
|
|
Hydatid serology Positive Negative N/A CT scan Ultrasound MRI X. ray Echocardiogram N/A |
139 (13.87%) 31 (3.09%) 832 (83.03%) 806 (80.44%) 475 (47.40%) 168 (16.77%) 69 (6.88%) 23 (2.29%) 105 (10.48%) |
|
Quantity of the cyst Single cyst Multiple cysts N/A |
466 (46.51%) 203 (20.26%) 333 (33.23%) |
|
Cyst status Patients with intact cysts Patients with ruptured cysts Patients with intact and ruptured cysts N/A |
100 (9.98%) 97 (9.68%) 6 (0.60%) 799 (79.74%) |
|
Type of treatment Surgical intervention Percutaneous treatment Medical treatment None N/A |
639 (63.77%) 75 (7.49%) 31 (3.09%) 2 (0.20%) 255 (25.45%) |
|
Medication Albendazole Albendazole & Praziquantel Mebendazole None N/A |
275 (27.44%) 9 (0.90%) 1 (0.10%) 26 (2.59%) 691 (68.96%) |
|
Follow up < 1 month – 6 months > 6 months – 1 year > 1 year – 2 years > 2years – 4 years > 4 years – 7 years > 7 years N/A |
347 (34.63%) 25 (2.50%) 27 (2.69%) 13 (1.30%) 5 (0.50%) 2 (0.20%) 583 (58.18%) |
|
Recurrence Yes No N/A |
26 (2.59%) 566 (56.49%) 410 (40.92%) |
|
Death Yes No N/A |
17 (1.70%) 666 (66.47%) 319 (31.83%) |
|
* Some patients had multiple clinical presentations, CT scan: computed tomography scan, MRI: magnetic resonance imaging, N/A: not available |
|
Discussion
Hydatidosis is most common in countries with extensive livestock industries but has recently become a significant global health issue due to rising immigration and travel [117, 232]. The disease is prevalent in Peru, Chile, Argentina, Uruguay, southern Brazil, the Mediterranean basin, Central Asia, western China, and East Africa. It remains absent in Antarctica and has been successfully eradicated through comprehensive control measures in Iceland, New Zealand, Tasmania, the Falkland Islands, and Cyprus [233]. In the present study, Spain unexpectedly showed the highest percentage of CE cases, with 36.13%, followed by China (26.95%) and Turkey (12.77%), collectively accounting for nearly 75% of all reported cases. Spain is known to be an endemic country for CE, but this unusually high percentage may be attributed to the fact that Spain has advanced healthcare infrastructure and diagnostic capabilities, which could lead to more accurate identification and reporting of CE cases. In contrast, in many developing countries, where resources and diagnostic tools may be limited, CE cases might be underreported or misdiagnosed [234]. This diversity underscores the importance of diagnostic and reporting capabilities when comparing CE prevalence across countries with differing healthcare systems. Regarding continental distribution, Asia represented 48.60% of cases, with Europe closely following at 45.91%. This distribution demonstrates that CE is not limited to traditionally endemic regions in developing countries but is also present in developed countries.
Studies have identified the liver as the most common site for hydatid cysts, accounting for 75% of cases, followed by the lungs (15%) and the brain (2%) [3]. Furthermore, cysts can form in various other organs and structures, including the abdominal and pleural cavities, kidneys, spleen, bones, eyes, ovaries, testes, and pancreas [233]. The current study's findings confirm that the liver remains the most frequently affected organ (73%), with the lungs (11%) being the second most common site, consistent with the literature. However, the current study found that the kidneys, heart, and muscles were more frequently affected than the brain (2%–4% of cases). This contrasts with previous studies identifying the brain as the third most commonly affected organ [3, 235].
The European Centre for Disease Prevention and Control (ECDC) indicates that the occurrence of echinococcosis does not display a notable difference between genders, presenting a nearly balanced male-to-female ratio of 1.1:1 [236]. This finding aligns with the results of the present study, where the gender distribution among the cases was nearly equal, with males comprising 50.39% and females 49.50%, yielding a male-to-female ratio of approximately 1:0.98. However, Otero-Abad et al. reported that women are more susceptible to echinococcosis than men. This increased risk was linked to their more significant participation in household activities, such as food preparation and caring for pets, heightening their exposure to infected dogs, soil, and vegetables [237].
Moro et al. stated that only 10-20% of CE cases are identified in patients under 16 years old [238]. This is likely because CE is slow-growing and often asymptomatic, with most liver and lung cysts becoming symptomatic and diagnosed in adults. In contrast, in the current study, the highest prevalence of CE was observed in the pediatric age group of 3-18 years, with a rate of 24.05% among the 262 patients with available age data. This difference may be attributed to advancements in early CE diagnosis and the fact that most cases in this study were based on case reports. However, it is important to note that age data were unavailable for 73.85% of patients, which could potentially influence the observed distribution, as the missing data might disproportionately affect certain age groups and alter the findings. The next highest prevalence was in the 19-30 years (19.85%) and 31-40 years (17.94%) age groups, indicating that CE is also common among young and middle-aged adults. In contrast, a study in Western Romania found the highest prevalence in individuals aged 50-59 years (21.7%) [239], while the current study showed a much lower prevalence in the 51-60 years age group (1.80%). These differences may be attributed to regional variations in risk factors, such as livestock exposure, environmental conditions, and access to healthcare, all of which can influence the age distribution of CE.
The clinical presentation of CE is highly variable, primarily influenced by factors such as the cyst's location, size, and condition. As CE cysts tend to grow slowly over time, they often result in a prolonged asymptomatic phase. Symptoms usually appear when the cysts reach a size that causes pressure effects or functional impairment in the affected organ [238]. Several studies highlight the differences in asymptomatic rates across various organ involvements. Ciftci et al. reported that 52.9% of patients with renal hydatid cysts were asymptomatic, indicating that cysts in the kidneys may remain unnoticed for extended periods until they cause local complications or are incidentally discovered [104]. In contrast, Akhan et al. found a higher rate of asymptomatic cases, 73.68%, among patients with liver hydatid cysts, suggesting that hepatic involvement might often go undetected, potentially due to the liver's capacity to accommodate growth without immediate symptoms [149]. In the present study, clinical presentation for 386 patients was available, and a much lower asymptomatic rate of 13.21% was observed. This discrepancy could be due to differences in cyst locations. It is possible that a higher proportion of patients in this study presented with symptoms due to the cysts being located in more clinically sensitive areas. Additionally, the lower asymptomatic rate might reflect a population with more advanced or larger cysts at the time of diagnosis, thereby increasing the likelihood of symptomatic presentation.
Early detection of CE can greatly improve the success of its management and treatment [240]. The definitive diagnosis of CE typically relies on imaging techniques such as radiology, ultrasound, computed tomography (CT), and magnetic resonance imaging (MRI) [241]. Serological tests like enzyme-linked immunosorbent assay (ELISA) offer high specificity for detecting HD, but a positive result does not accurately reveal the cyst’s location. Conversely, imaging methods provide detailed visualization, identifying cysts at specific sites. This limitation emphasizes combining serological testing with imaging to diagnose and precisely locate the hydatid cyst [242]. In the present study, among the 170 patients with CE who had serological test results available, 18.23% tested negative.
Preventing CE relies on disrupting E. granulosus's life cycle. For instance, regular screening and treatment of infected dogs have effectively eradicated the disease in endemic regions. Additional control measures include restricting the feeding of home-slaughtered livestock to dogs and vaccinating intermediate hosts, such as sheep [243]. Community education plays a crucial role in preventing disease spread by raising awareness of the risks associated with infected animals and contaminated environments. Ongoing monitoring and collaboration among healthcare providers, veterinarians, and the community are essential for early detection and prompt intervention [244].
One limitation of this study is the predominance of case reports among the included studies. While these reports offer valuable insights into rare occurrences, they are inherently limited by small sample sizes, and potential selection bias. As a result, the findings may not be easily generalized to broader populations, and the ability to draw strong conclusions. Further research is needed to address the diagnostic challenges of CE in non-endemic regions, with a focus on improving early detection and treatment. Future studies should prioritize increasing healthcare professionals' knowledge, refining diagnostic processes, and evaluating the effectiveness of serological and imaging tools in regions with low disease prevalence.
Conclusion
Hydatidosis persists as a significant global public health concern, impacting both developing and developed countries. The liver and lungs remain the primary sites of infection. Preventive strategies, including regular animal screening and enhanced public health education, are essential for controlling the spread of the disease.
Declarations
Conflicts of interest: The author(s) have no conflicts of interest to disclose.
Ethical approval: Not applicable.
Consent for participation: Not applicable.
Consent for publication: Not applicable.
Funding: The present study received no financial support.
Acknowledgments: None to be declared.
Authors' contributions: HAN, BAA, FHK, and HOA: major contributors to the conception of the study, as well as the literature search for related studies, and manuscript writing. SMA, SHM, RQS FA, YMM and DAH: Literature review, design of the study, critical revision of the manuscript, and processing of the tables. TMM, MNH, HAH, SHK, KKM, DAO, SHS and KAN: Literature review, data analysis and interpretation. All authors have read and approved the final version of the manuscript.
Use of AI: AI was not used in the drafting of the manuscript, the production of graphical elements, or the collection and analysis of data.
Data availability statement: Not applicable.
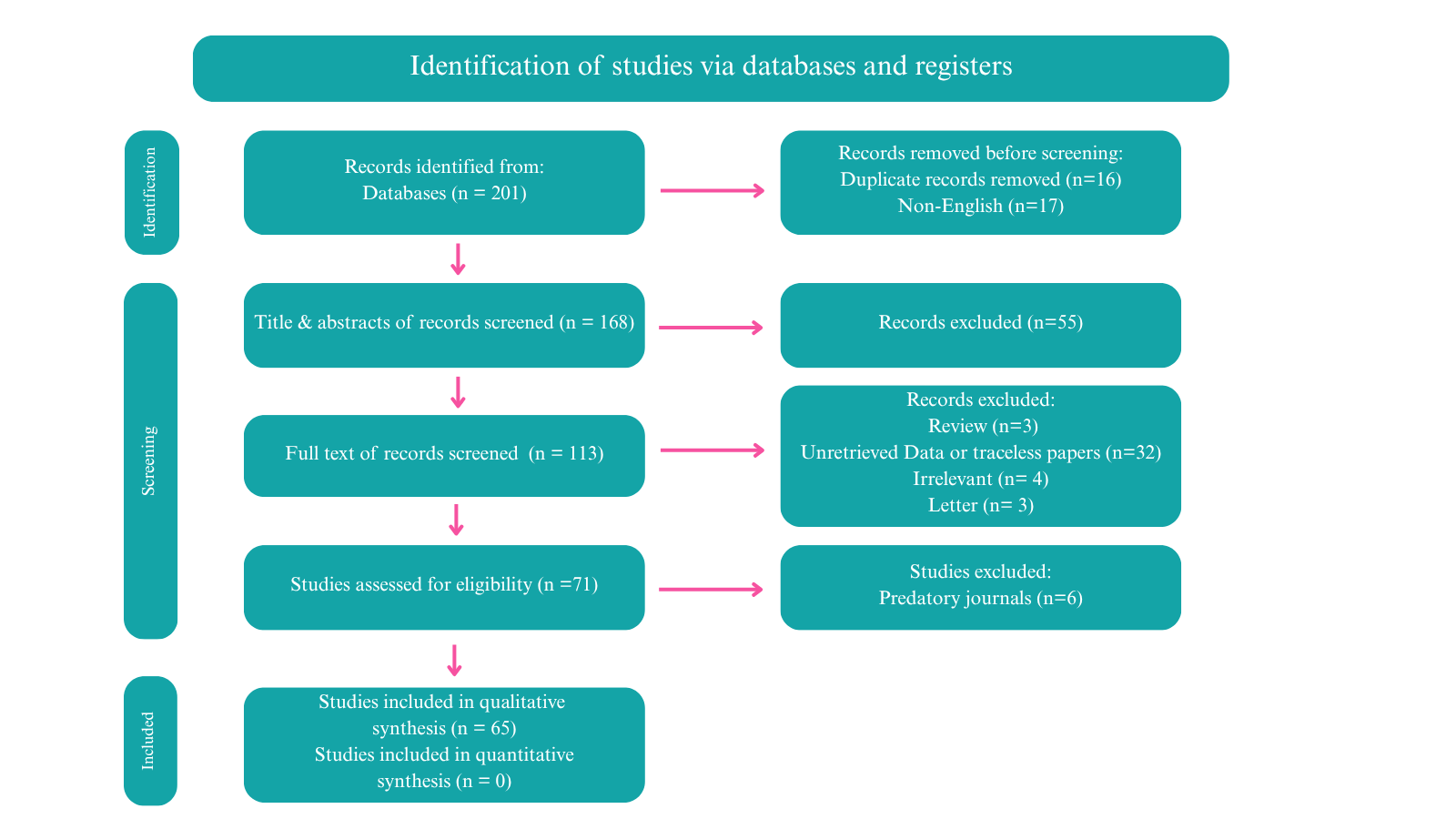
Blunt Chest Trauma and Chylothorax: A Systematic Review
Hiwa O. Abdullah, Fahmi H. Kakamad, Harem K. Ahmed, Bnar J. Hama Amin, Hadi M. Abdullah, Shvan H....
Abstract
Introduction: Although traumatic chylothorax is predominantly associated with penetrating injuries, instances following blunt trauma, as a rare and challenging condition, are being increasingly documented. This study aims to systematically review the reported cases of blunt chest traumatic chylothorax (BCTC) and provide comprehensive insights into the condition.
Methods: Related studies published until December 11, 2024, were identified through Google Scholar. All studies documenting instances of BCTC, without restriction on cause or patient demographics, were included. Studies were excluded if they focused on chylothorax caused by penetrating injuries, their content was unretrievable, they were review articles, or they were published in blacklisted journals.
Results: Sixty-five eligible studies, encompassing 69 cases of BCTC, were included in the review. It predominantly affected males (73.91%), with patient ages ranging from 11 months to 84 years old. The most common clinical findings were dyspnea (47.83%) and abnormal auscultation or percussion (34.78%), with road traffic accidents as the primary cause (59.42%). Unilateral chylothorax was found in 72.46% of cases, bilateral chylothorax occurred in 27.54%, and pleural effusion was the most frequent radiological finding (55.07% in X-ray and 33.33% in computed tomography). Treatment typically included drainage (94.20%), parenteral nutrition (50.72%), and thoracic duct closure (39.13%). Most patients achieved complete recovery (89.85%), and six cases (8.70%) died.
Conclusion: The condition is rare and complex, underscored by the wide variability in patient demographics, clinical presentations, chylothorax onset, and management approaches. Given the challenges posed by limited evidence, the findings emphasize the need for early recognition and individualized management strategies.
Introduction
Chylothorax is a rare condition characterized by the accumulation of chyle in the pleural cavity caused by a disruption of the thoracic duct [1]. Chyle is an opalescent fluid that consists of triglycerides, chylomicrons, proteins, electrolytes, immunoglobulins, and fat-soluble vitamins, transported from the gastrointestinal system into the bloodstream by the thoracic duct. It makes up about 1-3% of total body weight in adults. Chylothorax was initially described by Bartolet in 1633 and later reported in the literature by Quinke in 1875 [1,2]. It is categorized into congenital, neoplastic, traumatic, and miscellaneous forms. The most common cause is malignancy, which leads to obstruction of the thoracic duct, while traumatic chylothorax is typically iatrogenic, resulting from surgical procedures or catheter placement. Penetrating trauma is the usual cause of traumatic chylothorax, while blunt trauma is considered an infrequent cause [1,2]. It may also develop due to chest compression or changes in intrathoracic pressure, such as during coughing or persistent vomiting [2].
The incidence of chylothorax is about 0.2% following blunt thoracic trauma and 0.9% after penetrating trauma. Bilateral chylothorax resulting from blunt trauma, mainly when no other injuries are evident, is an infrequent but severe complication [3]. Without prompt treatment, chylothorax can lead to serious complications, such as cardiopulmonary distress and significant nutritional deficiencies, with a high mortality rate of up to 15.5% [2-4]. Although traumatic chylothorax is predominantly associated with penetrating injuries, instances following blunt trauma have been increasingly documented, highlighting the need for awareness among healthcare providers regarding this potential complication [5,6]. This study aims to systematically review the reported cases of blunt chest traumatic chylothorax (BCTC) and provide comprehensive insights into the condition.
Methods
Literature search
The study followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. Related studies published until December 11, 2024, were identified through Google Scholar using a search strategy that combined the following keywords with the “allintitle” and “including citation” features: (blunt trauma chylothorax), (blunt thoracic trauma chylothorax), (blunt thoracic injury chylothorax), (blunt chest injury chylothorax), (blunt torso trauma chylothorax), (blunt thoracic duct trauma), (blunt thoracic duct injury) and (traumatic chylothorax). The search was limited to English-language publications.
Eligibility criteria
All studies or reports documenting instances of BCTC, without restriction on cause or patient demographics, were eligible for inclusion. Studies were excluded if they focused on chylothorax caused by factors other than blunt chest trauma, if their content was unretrievable, if they were review articles, or if they were published in blacklisted journals. The legitimacy of the studies was verified by cross-referencing with widely recognized predatory journal checklists [7].
Study selection
First, an author conducted a literature search using the specified keywords and collected the relevant results. The titles and abstracts of the identified studies were then screened to exclude duplicates, non-English studies, and those unrelated to the study objective. Full-text screening was conducted for studies that passed the initial filtration, excluding those with unretrievable content or irrelevant study designs, such as reviews. This step was supervised by two authors, who independently reviewed each study. Finally, the remaining studies underwent legitimacy filtering.
Data extraction
The collected data encompassed various parameters, including the first author's name, year of publication, patient demographics, clinical manifestations, causes of chylothorax, chyle volume and content, the onset of chyle production, diagnostic methods, ICU admission status, treatment modalities, outcomes, and follow-up.
Statistical Analysis
The extracted data were organized in an Excel sheet (2019) and analyzed descriptively using the Statistical Package for the Social Sciences (SPSS, v. 27, IBM Co.). The results were presented in frequencies with percentages, means with standard deviation, and ranges.
Results
Study identification
A systematic search yielded 201 studies, all of which were case reports. After removing duplicates (16) and non-English articles (17), 168 titles and abstracts were screened. Fifty-five case reports were excluded due to irrelevance, and full-text evaluation of the remaining 113 case reports led to the exclusion of an additional 42. Furthermore, six articles were excluded for being published in warning-listed journals. Consequently, 65 eligible case reports, encompassing 69 cases of BCTC, were included in the review [1-6,8-66] (Tables 1 and 2). The identification process is outlined in a PRISMA flowchart (Figure 1).
|
First author, year [Reference] |
Country |
Age (year) |
Gender |
CFP |
Cause |
SOC |
Amount of chyle (ml)/day* |
COAP (day) |
Biochemical content of chyle |
|
Harvey, 2024 [5] |
USA |
60 |
F |
Chest pain, multiple rib fractures |
RTA |
Left |
<500 |
2 |
Triglycerides |
|
Burduniuc, 2023 [2] |
Czech Republic |
70 |
F |
Blunt injury |
Fall on stairs |
Right |
>1000-2000 |
3 |
Protein, cholesterol, triglycerides |
|
Dung, 2023 [14] |
Vietnam |
32 |
M |
Thoracic spine injury, paraplegia |
RTA |
Right |
>1000-2000 |
At once |
Cholesterol, triglycerides |
|
Kim, 2023 [4] |
South Korea |
45 |
M |
Hemodynamically unstable, chest discomfort, multiple fractures, hemopneumothorax |
Crushed by a 2-ton metal frame |
Left |
>1000-2000 |
1.66 |
Triglycerides |
|
Boateng 2023 [33] |
USA |
75 |
F |
Respiratory distress |
Fall from bed |
Right |
<500 |
At once |
Triglycerides |
|
Ruest 2023 [34] |
USA |
15 months |
M |
Tenderness over right paraspinal thoracolumbar back, abnormal auscultation |
Child abuse |
Right |
N/A |
At once |
N/A |
|
Mohanakrishnan 2022 [35] |
USA |
70 |
F |
Dyspnea, back pain, abnormal auscultation |
Violent coughing episode |
Right |
>1000-2000 |
At once |
Chylomicrons, triglycerides |
|
Mazhar, 2021[23] |
UK |
42 |
F |
Dyspnea, abnormal auscultation |
Fall from horse 1 week before presentation |
Right |
>1000-2000 |
7 |
Triglycerides |
|
Waseem, 2021[32] |
Pakistan |
50 |
M |
Dyspnea |
RTA 2 days before presentation |
Bilateral |
>1000-2000 |
2 |
Triglycerides, cholesterol, fat-rich fluid with few inflammatory cells |
|
Din Dar 2021 [36] |
India |
50 |
M |
Blunt injury |
RTA |
Right |
>1000-2000 |
25 |
Triglyceride, chylomicrons |
|
Bacon, 2020 [9] |
USA |
53 |
M |
Hemopneumothorax |
RTA |
Left |
<500 |
5 |
N/A |
|
Champion, 2020 [12] |
Canada |
29 |
M |
Dyspnea, flushing, diaphoresis, vomiting, abnormal auscultation |
RTA |
Bilateral |
>1000-2000 |
At once |
Cholesterol, triglycerides |
|
Jindal 2019 [37] |
India |
35 |
M |
Dyspnea, respiratory distress |
RTA |
Bilateral |
>1000-2000 |
4 |
Triglyceride, WBC, albumin, glucose, protein, LDH |
|
Ahmed, 2018 [1] |
Iraq |
42 |
M |
Severe back pain |
RTA |
Right |
500-1000 |
2 |
Triglycerides and lymphocyte |
|
Brown, 2018 [10] |
USA |
53 |
M |
Thoracoabdominal injuries, subcutaneous emphysema, unstable pelvis |
RTA |
Left |
>1000-2000 |
N/A |
Triglycerides and lymphocyte |
|
Litzau, 2018 [22] |
USA |
66 |
F |
Dyspnea, multiple fractures, abnormal auscultation |
RTA 7 days before presentation |
Right |
>1000-2000 |
7 |
Triglycerides |
|
Kozul, 2017 [19] |
Australia |
18 |
M |
Multiple injuries |
RTA |
Bilateral |
500-1000 |
0.46 |
N/A |
|
Lee, 2017 [21] |
South Korea |
70 |
M |
Hemothorax, flail chest |
RTA |
Right |
>2000 |
5 |
Triglycerides, cholesterol |
|
Mohamed, 2017 [3] |
USA |
51 |
M |
Dyspnea, chest pain, abnormal auscultation |
Fall on stairs |
Bilateral |
>1000-2000 |
5 |
Triglycerides, Leukocytes, RBCs, LDH, protein |
|
Spasić, 2017 [6] |
Serbia |
55 |
F |
Multiple injuries |
RTA |
Right |
>2000 |
5 |
N/A |
|
Sriprasit, 2017 [31] |
Thailand |
27 |
F |
Hemothorax, neurogenic shock, multiple fractures |
RTA |
Left |
<500 |
5 |
Triglycerides, protein, glucose, LDH |
|
Hara 2017 [38] |
Japan |
17 |
F |
Breathing difficulty, abnormal percussion |
Recurrent chylothorax, physical punishment |
Left |
500-1000 |
At once |
N/A |
|
Jahn 2017 [39] |
Germany |
8 |
F |
Respiratory distress, abnormal percussion, and auscultation |
Pedestrian hit by a motor vehicle |
Left |
<500 |
5 |
Protein, albumin, LDH, triglycerides, cholesterol |
|
Ghodrati 2016 [40] |
Iran |
12 |
F |
Dyspnea, respiratory distress |
Chest trauma during play at school |
Bilateral |
N/A |
N/A |
N/A |
|
Lee 2016 [41] |
South Korea |
50 |
M |
Paraplegia |
Fall from height during construction work |
Right |
>1000-2000 |
3 |
Triglycerides |
|
Sendama 2015 [42] |
UK |
84 |
F |
Dyspnea, abnormal auscultation |
Fall |
Right |
500-1000 |
4 |
Protein, LDH, cholesterol, triglycerides |
|
Snow 2015 [43] |
USA |
22 months |
M |
Cough, dyspnea, respiratory distress, altered mental status, abnormal auscultation |
Fall from a chair |
Right |
<500 |
2 |
Triglycerides |
|
Adams 2013 [44] |
USA |
73 |
M |
Paraplegia, rib fractures, hemothorax |
RTA |
Right |
N/A |
9 |
Triglycerides, lymphocytes, glucose, LDH, lipemia |
|
Kumar 2013 [45] |
India |
32 |
M |
Blunt injury, fracture of right femur |
RTA |
Right |
>1000-2000 |
2 |
Triglycerides, chylomicrons |
|
23 |
M |
Hemopneumothorax, multiple rib fractures, subcutaneous emphysema |
RTA |
Right |
500-1000 |
1 |
Triglycerides |
||
|
40 |
M |
Hemothorax |
RTA |
Right |
500-1000 |
2 |
Triglycerides |
||
|
Sharkey 2012 [46] |
UK |
50 |
M |
Multiple fractures, hematoma, hemothorax, pneumothorax |
RTA |
Right |
500-1000 |
N/A |
Triglyceride, cholesterol |
|
Sokouti, 2011[30] |
Iran |
15 |
M |
Respiratory distress, dyspnea, back pain, abnormal auscultation |
Fall 11 years ago |
Bilateral |
>2000 |
40 |
Triglycerides, protein, cholesterol, fat |
|
Kurklinsky 2011 [47] |
USA |
26 |
F |
Pleuritic chest pain |
Water-skiing fall |
Bilateral |
>1000-2000 |
2 |
Triglycerides |
|
Apostolakis, 2009 [8] |
USA |
75 |
F |
Dyspnea, back pain |
RTA |
Bilateral |
500-1000 |
At once |
Protein, LDH, glucose, amylase, triglycerides, cholesterol, albumin, globulin, K, Na, lymphocytes, erythrocytes |
|
22 |
M |
Back pain, hematoma of left thigh, chest pain |
RTA |
Bilateral |
<500 |
0.25 |
Protein, LDH, glucose, amylase, triglycerides, cholesterol, albumin, globulin, K, Na, lymphocytes, erythrocytes |
||
|
Huber, 2009 [16] |
USA |
47 |
M |
Dyspnea, chest pain |
Crushed by multiple metal gates |
Bilateral |
500-1000 |
3 |
Triglycerides |
|
Schurz, 2009 [28] |
Austria |
39 |
M |
Dyspnea, thoracodorsal pain |
RTA |
Left |
>1000-2000 |
14 |
N/A |
|
Serin-Ezer, 2009 [29] |
Turkey |
4 |
M |
Dyspnea, somnolence, abnormal auscultation |
Hit by a manufacturing pipe falling from a truck |
Bilateral |
<500 |
At once |
Triglycerides, cholesterol, protein, LDH, glucose |
|
Kamiyoshihara, 2008 [18] |
Japan |
51 |
M |
Dyspnea, dullness in percussion |
RTA 20 years before presentation |
Bilateral |
>1000-2000 |
At once (but the trauma dated back to 20 years prior)
|
Triglycerides |
|
Pandey 2008 [48] |
Australia |
36 |
M |
Chest pain, flail chest, hypotension |
Fall from balcony |
Right |
>1000-2000 |
2 |
N/A |
|
Lee, 2006 [20] |
South Korea |
11 |
M |
Dyspnea, nausea, vomiting, abdominal discomfort, abnormal auscultation |
RTA 3 days before presentation |
Bilateral |
N/A |
3 |
Triglycerides, cholesterol, protein |
|
Ozcelik, 2004 [26] |
Turkey |
15 |
F |
Respiratory distress, subcutaneous emphysema, pneumothorax |
Trapping under rubble during a 7.8 magnitude earthquake |
Right |
N/A |
45 |
Cholesterol, triglycerides |
|
Robbins 2004 [49] |
USA |
41 |
M |
Chest injury, refractory hiccups, nausea |
RTA |
Bilateral |
N/A |
N/A |
N/A |
|
Buchan 2001 [50] |
UK |
18 |
M |
Dyspnea |
RTA |
Right |
>1000-2000 |
4 |
N/A |
|
Chamberlain, 2000 [11] |
UK |
29 |
M |
Pneumothorax, abdominal and paraspinal pain, loss of motor power, and sensation below T12/L1 |
RTA |
Right |
>1000-2000 |
0.88 |
N/A |
|
Glyn-Jones 2000 [51]
|
UK |
28 |
M |
Dyspnea, polytrauma, tachypnea |
RTA |
Left |
>2000 |
N/A |
Triglyceride, cholesterol, WBC |
|
Golden, 1999 [15] |
USA |
53 |
F |
Chest pain, multiple fractures, hemopneumothorax, abnormal auscultation |
RTA |
Left |
>2000 |
6 |
Triglycerides |
|
McCormick, 1999 [24] |
USA |
46 |
M |
Chest pain, dyspnea, abnormal auscultation, dullness to percussion |
Hit-and-run motor vehicle accident |
Bilateral |
>1000-2000 |
14 |
Protein, cholesterol, triglycerides |
|
Ikonomidis, 1997 [17] |
Canada |
17 |
M |
Closed head injury, multiple fractures, respiratory distress, tracheal hematoma |
RTA |
Bilateral |
<500 |
At once |
Triglycerides |
|
24 |
M |
Closed head injury, rib fractures, hemothorax |
Snowboarding accident |
Left |
<500 |
At once |
Triglycerides |
||
|
Guleserian, 1996 [52] |
USA |
11 months |
M |
Dyspnea, coughing, cold symptoms, grunting, abnormal percussion |
Child abuse |
Right |
500-1000 |
N/A |
Triglycerides, cholesterol, WBC |
|
Milano, 1994 [25] |
Italy |
26 |
F |
Dyspnea |
Fall while skiing 4 months prior |
Left |
>1000-2000 |
50 |
Triglycerides |
|
Fogli, 1993 [53] |
Italy |
31 |
M |
Suspected traumatic hemothorax, dyspnea, cough |
RTA |
Right |
500-1000 |
N/A |
N/A |
|
Grant, 1991 [54] |
New Zealand |
32 |
M |
Dyspnea, chest and back pain |
RTA |
Right |
>1000-2000 |
N/A |
N/A |
|
Dulchavsky, 1988 [13] |
USA |
48 |
M |
Dyspnea, chest pain, abnormal auscultation |
Fistfight |
Right |
>1000-2000 |
At once |
Cholesterol, HDL, triglycerides, pre-beta lipoprotein, chylomicrons |
|
Brook 1988 [55] |
USA |
27 |
M |
Respiratory distress, abnormal percussion, tachycardia |
RTA |
Bilateral |
>2000 |
3 |
Triglycerides
|
|
Pai, 1984 [27] |
USA |
19 |
M |
Neck, back, and chest pain |
RTA |
Right |
>1000-2000 |
N/A |
N/A |
|
Krishnan 1982 [56] |
Malaysia |
29 |
M |
Dyspnea, abnormal percussion |
RTA |
Right |
>2000 |
2 |
N/A |
|
Azambuja 1981 [57] |
Brazil |
42 |
M |
Paraplegia, hemopneumothorax |
RTA |
Right |
N/A |
3 |
N/A |
|
Rea 1960 [58] |
UK |
28 |
M |
Dyspnea, apex beat displaced to the left |
Crush injury from falling planks |
Right |
500-1000 |
4 |
Lipid, protein, RBC, lymphocytes |
|
Guest 1955 [59] |
Canada |
19 |
M |
Dyspnea, dry cough, tachypnea, dull percussion |
RTA |
Right |
>1000-2000 |
26 |
N/A |
|
Elliot 1948 [60] |
Canada |
56 |
M |
Fall injury, paraplegia, respiratory distress |
Fall from a tree |
Right |
500-1000 |
3 |
Fat |
|
Dorsey 1942 [61] |
USA |
60 |
M |
Alcoholic stupor, dyspnea, chest pain, abnormal percussion |
Fall down a flight of stairs |
Right |
>2000 |
0.5 |
Protein, albumin, globulin, fat |
|
Cellan-Jones 1940 [62] |
UK |
32 |
M |
Dyspnea, chest tightness |
A stone hitting the chest and dorsal spine striking a block of coal |
Right |
>1000-2000 |
3 |
Fat |
|
Brown 1937 [63] |
USA |
N/A |
F |
Respiratory distress, abdominal distention |
RTA |
Bilateral |
>1000-2000 |
At once |
N/A |
|
Bauersfeld 1937 [64] |
USA |
22 |
M |
Breathing difficulty, laceration of the scalp, pain in lower abdomen and lumbar region, cyanosis, cold extremities |
RTA |
Right |
>2000 |
8 |
Fat globules |
|
Lillie 1935 [65] |
USA |
45 |
M |
Blunt injury |
Fall from a scaffold 20 feet high |
Right |
>2000 |
N/A |
N/A |
|
Macnab 1932 [66] |
Canada |
46 |
M |
Chest and back pain, dullness percussion, dyspnea, anorexia, weakness, intermittent fever, hypotension |
Fall from a height of 11 feet |
Right |
500-1000 |
6 |
N/A |
|
F: female, M: male, CFP: clinical findings & presentation, SOC: Side of chylothorax, hr: hour, N/A: non-available, COAP: Chyle onset after presentation, RTA: road traffic accident, RBC: red blood cell, LDH: lactate dehydrogenase, HDL: high density lipoprotein, WBC: white blood cell. * The amount of chyle has been grouped rather than the actual amount. |
|||||||||
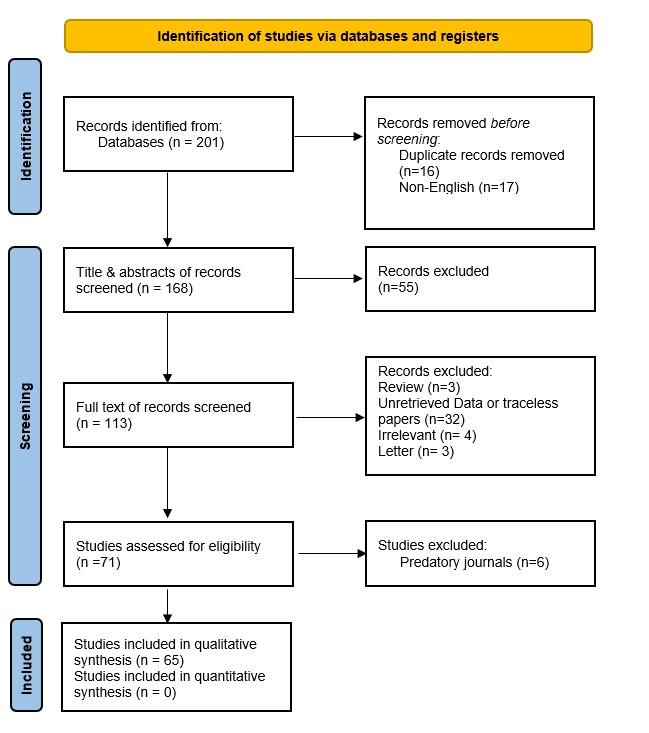
|
First author, year [Reference] |
Chest X-ray |
CT |
MRI |
ICU admission |
Treatment |
Thoracic duct ligation approach |
Mode of drainage |
Duration of chest tube placement (day) |
Follow-up (weeks) |
Outcome |
|
Harvey, 2024 [5] |
Pleural effusion |
Hemopneumothorax, pneumomediastinum, retrosternal hematoma, multiple rib fracture, lung contusions, and manubrium fractures |
N/A |
Yes |
Drainage, medium chain fatty acid diet |
N/A |
Chest tube |
7 |
8 |
Recovered |
|
Burduniuc, 2023 [2] |
Pleural effusion, multiple rip fracture |
Pleural effusion, multiple rib fracture |
Th12 vertebral fracture |
Yes |
Drainage, thoracic duct ligation |
Thoracotomy |
Chest tube |
N/A |
N/A |
Recovered |
|
Dung, 2023 [14] |
Pleural effusion |
T9 and T10 vertebral fracture |
N/A |
No |
Drainage, octreotide, TPN, thoracic duct embolization |
2.7 Fr microcatheter, fluoroscopic guidance |
Chest tube |
7 |
N/A |
Recovered |
|
Kim, 2023 [4] |
Pleural effusion |
Lipiodol leakage near T10–11 level |
N/A |
Yes |
Drainage, TPN, intranodal lymphangiography, therapeutic lipiodol injection |
N/A |
Chest tube |
39 |
N/A |
Recovered |
|
Boateng 2023 [33] |
N/A |
Pleural effusion, lung collapse |
N/A |
No |
Drainage, medium-chain triglyceride |
N/A |
Chest tube |
N/A |
N/A |
Died |
|
Ruest 2023 [34] |
Pleural effusion |
T12 vertebral body fracture, rib fractures |
N/A |
Yes |
Drainage |
N/A |
Chest tube |
N/A |
N/A |
Recovered |
|
Mohanakrishnan 2022 [35] |
N/A |
Pleural effusion, minimal ascites |
N/A |
No |
Drainage, octreotide, low-fat diet, NPO, TPN, pleurodesis, thoracic duct embolization |
Coiling and glue embolization |
Chest tube |
N/A |
N/A |
Recovered |
|
Mazhar, 2021[23] |
Pleural effusion |
Pleural effusion, T10 spinous process fracture |
N/A |
No |
Drainage, octreotide, medium-chain triglyceride diet |
N/A |
Chest tube |
3 |
N/A |
Recovered |
|
Waseem, 2021[32] |
Pleural effusion |
Pleural effusion |
N/A |
No |
Only drainage |
N/A |
Chest tube |
5 |
N/A |
Recovered |
|
Din Dar 2021 [36] |
N/A |
Multiple rib fractures, hemothorax |
N/A |
No |
Drainage, NPO, TPN, octreotide, thoracic duct embolization |
Thoracotomy |
Chest tube |
25 |
48 |
Recovered |
|
Bacon, 2020 [9] |
Multiple rib fracture |
Multiple rib fracture |
N/A |
Yes |
Drainage, free-fat diet |
N/A |
Chest tube |
N/A |
12 |
Recovered |
|
Champion, 2020 [12] |
Pleural effusion |
Pleural effusion |
N/A |
No |
Drainage, octreotide, TPN, thoracic duct ligation |
Thoracotomy |
Chest tube |
N/A |
6 |
Recovered |
|
Jindal 2019 [37] |
Pleural effusion |
Multiple rib fractures, lung contusions, fracture of L1 and L2 vertebrae |
N/A |
Yes |
Drainage, thoracic duct ligation, TPN, octreotide, fat-free and medium chain triglyceride |
Thoracotomy |
Chest tube |
8 |
8 |
Recovered |
|
Ahmed, 2018 [1] |
Opacification of hemithorax |
D10 vertebral fracture, multiple rib fracture |
N/A |
Yes |
Drainage, low-fat diet, albumin vial, octreotide |
N/A |
Chest tube |
|
|
|
|
Brown, 2018 [10] |
N/A |
Left temporal epidural hematoma, pulmonary contusions, multiple skeletal fractures, pneumomediastinum compressing the right atrium |
Not mentioned the findings |
No |
Drainage, NPO, TPN, octreotide, thoracic duct embolization, and ligation |
Thoracotomy, decortication |
Chest tube |
|
|
|
|
Litzau, 2018 [22] |
Pleural effusion |
Pleural effusion |
N/A |
No |
Drainage, low-fat diet |
N/A |
Chest tube |
|
|
|
|
Kozul, 2017 [19] |
N/A |
Hemopneumothorax, mediastinal shift to the right, pleural effusion |
N/A |
No |
Drainage, No fat/low-fat diet |
N/A |
Chest tube |
|
|
|
|
Lee, 2017 [21] |
Pleural effusion |
Multiple rib fracture, hemopneumothorax (left), subcutaneous emphysema (left), and atelectasis (right). |
N/A |
Yes |
Drainage, TPN, NPO, fat-free diet, medium-chain lipid diet, thoracic duct ligation, pleurectomy |
Thoracotomy |
Chest tube |
|
|
|
|
Mohamed, 2017 [3] |
Obliteration of left costophrenic angle (pleural effusion) |
Bilateral effusion |
N/A |
No |
Drainage, fat-free diet with medium-chain triglycerides, octreotide |
N/A |
Thoracentesis |
|
|
|
|
Spasić, 2017 [6] |
Lung contusion |
Rib and thoracic vertebral fracture, hydropneumothorax, lung contusion, pneumomediastinum |
N/A |
No |
Drainage, TPN, thoracic duct suturing |
Thoracotomy |
Chest tube |
|
|
|
|
Sriprasit, 2017 [31] |
N/A |
N/A |
N/A |
Yes |
Drainage, NPO, TPN |
N/A |
Chest tube |
|
|
|
|
Hara 2017 [38] |
Pleural effusion |
N/A |
N/A |
No |
Drainage, low-fat diet with medium-chain triglycerides, intranodal lymphangiography with lipiodol |
N/A |
Chest tube |
|||
|
Jahn 2017 [39] |
Pulmonary opacification |
Lung contusions |
N/A |
No |
Drainage, fat-free diet |
N/A |
Chest tube |
|||
|
Ghodrati 2016 [40] |
Pleural effusion |
N/A |
N/A |
Yes |
Drainage, thoracic duct embolization |
Unknown |
Chest tube |
|||
|
Lee 2016 [41] |
N/A |
Incomplete cord injury at the thoracic spinal vertebrae (T10 and T11) |
N/A |
No |
Drainage, TPN, NPO, thoracic duct ligation |
VATS |
Chest tube |
|||
|
Sendama 2015 [42] |
Pleural effusion |
Multisegment fracture of L1 vertebra |
N/A |
No |
Drainage, medium chain fatty acid diet, octreotide |
N/A |
Chest tube |
|||
|
Snow 2015 [43] |
Opacification of right chest, mediastinal shift to left |
N/A |
N/A |
Yes |
Drainage, NPO, TPN, octreotide, low-fat diet |
N/A |
Chest tube |
|||
|
Adams 2013 [44] |
Pleural effusion, atelectasis |
Pleural effusion, atelectasis |
N/A |
Yes |
Drainage, NPO, TPN, octreotide |
N/A |
Thoracentesis, chest tube |
|||
|
Kumar 2013 [45] |
N/A |
Pleural effusion, multiple rib fractures |
N/A |
No |
Drainage, NPO, TPN, octreotide, chest physiotherapy |
N/A |
Chest tube |
|||
|
N/A |
Hemopneumothorax, multiple rib fractures |
N/A |
No |
Drainage, NPO, TPN, octreotide, chest physiotherapy |
N/A |
Chest tube |
||||
|
N/A |
Bilateral hemothorax, lung contusion |
N/A |
Yes |
Drainage, NPO, TPN, octreotide, exploratory laparotomy for biliary leak |
N/A |
Chest tube |
||||
|
Sharkey 2012 [46] |
N/A |
N/A |
N/A |
Yes |
Drainage, NPO, TPN, octreotide, medium fatty acid diet |
N/A |
Chest tube |
|||
|
Sokouti, 2011[30] |
Large cystic mass in left posterior mediastinum |
Large low-density cystic mass in the left posterior mediastinum, left pleural effusion |
N/A |
No |
Drainage, thoracic duct ligation, TPN |
Laparotomy, Thoracotomy |
Chest tube |
|||
|
Kurklinsky 2011 [47] |
N/A |
Pleural effusion, dilated cisterna chyli, middle mediastinum fluid collection |
N/A |
No |
Drainage, TPN, thoracic duct embolization |
3 Fr microcatheter with ultrasound guidance |
Thoracentesis |
|||
|
Apostolakis, 2009 [8] |
Pleural effusion |
Pleural effusion |
N/A |
No |
Drainage, starvation diet, TPN |
N/A |
Chest tube |
|||
|
Pleural effusion, rib fractures, ipsilateral sternoclavicular joint dislocation |
Lung contusion |
N/A |
No |
Drainage, starvation diet, TPN |
N/A |
Chest tube |
||||
|
Huber, 2009 [16] |
Pleural effusion |
Pleural effusion, right pneumothorax, multiple rib fracture, aortic pseudoaneurysm, retrocrural hemorrhage |
N/A |
Yes |
Drainage, thoracic duct ligation, medium chain fatty acid diet, mechanical pleurodesis |
Thoracotomy |
Chest tube |
|||
|
Schurz, 2009 [28] |
Multiple rib fracture, pleural effusion |
Pleural effusion |
Osseous lesions and pleural effusion |
Yes |
Drainage, TPN, fat-free diet, plain tea, apple puree |
N/A |
Pleural puncture, chest tube |
|||
|
Serin-Ezer, 2009 [29] |
Multiple rib fracture, pleural effusion |
Pleural effusion |
N/A |
No |
Drainage, NPO, TPN |
N/A |
Chest tube |
|||
|
Kamiyoshihara, 2008 [18] |
Pleural effusion |
Pleural effusion |
N/A |
No |
Drainage, low-fat diet, TPN, thoracic duct ligation, pleurodesis |
Thoracotomy |
Thoracentesis, Chest tube |
|||
|
Pandey 2008 [48] |
N/A |
Hemopneumothorax, pulmonary contusion, multiple rib fractures, pneumomediastinum |
N/A |
Yes |
Drainage, octreotide, thoracic duct ligation |
Laparoscopic ligation |
Chest tube |
|||
|
Lee, 2006 [20] |
Elevation of diaphragms, cardiomegaly |
Pleural effusion, massive ascites around liver and spleen |
N/A |
No |
Drainage, medium-chain lipid solution, NPO |
N/A |
Thoracentesis, chest tube |
|||
|
Ozcelik, 2004 [26] |
Pneumothorax, consolidated right lung, pleural effusion |
Right lung consolidation, pleural effusion |
N/A |
No |
Drainage, thoracic duct mass ligation, TPN |
Thoracotomy |
Chest tube |
|||
|
Robbins 2004 [49] |
N/A |
Pleural effusion, focal fluid collection |
N/A |
No |
EUS-guided aspiration, injection of sodium morrhuate |
N/A |
Aspiration |
|||
|
Buchan 2001 [50] |
Pleural effusion |
N/A
|
N/A |
No |
Drainage, low-fat diet, medium-chain triglycerides, thoracic duct ligation |
Thoracotomy |
Chest tube |
|||
|
Chamberlain, 2000 [11] |
Pneumothorax, hemithorax opacification |
Free abdominal gas |
Fractures of T4 and T10 with spinal cord contusion and hematoma |
No |
Drainage, TPN, NPO, Supradiaphragmatic duct ligation |
Thoracotomy |
Chest tube |
|||
|
Glyn-Jones 2000 [51]
|
Mediastinal shift |
Minor anterior wedge fractures at T5 and T10 |
Cord injury at T10 |
No |
Drainage, thoracic duct ligation, pleurodesis, fat-free diet |
Thoracotomy |
Chest tube |
|||
|
Golden, 1999 [15] |
N/A |
N/A |
N/A |
Yes |
Drainage, TPN, NPO, thoracic duct ligation |
Thoracotomy |
Chest tube |
|||
|
McCormick, 1999 [24] |
Pleural effusion |
Disruption of the thoracic duct at the T5 level |
N/A |
No |
Only drainage |
N/A |
Chest tube |
|||
|
Ikonomidis, 1997 [17] |
Pneumomediastinum, pulmonary contusions |
N/A |
N/A |
No |
Drainage, TPN, bowel rest |
N/A |
Chest tube |
|||
|
Left hemothorax |
Left mediastinal hematoma, T3 vertebral fracture |
N/A |
No |
Drainage, TPN, bowel rest |
N/A |
Chest tube |
||||
|
Guleserian, 1996 [52] |
Right lung opacification and mediastinal shift to left |
N/A |
N/A |
No |
Drainage, nasogastric feeding with medium-chain triglycerides, low-fat diet |
N/A |
Chest tube |
|||
|
Milano, 1994 [25] |
Pleural effusion |
Dense lymphatic opacification at L1-L2, chyloma at D11, pleural leakage from left duct |
N/A |
No |
Drainage, low-fat diet, medium-chain triglycerides, TPN, pleuroperitoneal shunt |
N/A |
Thoracentesis |
|||
|
Fogli, 1993 [53] |
Pleural effusion, mediastinal shift |
N/A |
N/A |
No |
Drainage, TPN |
N/A |
Chest tube |
|||
|
Grant, 1991 [54] |
Pleural effusion |
N/A |
N/A |
No |
Drainage, thoracic duct ligation, TPN, low-fat diet |
Thoracotomy |
Thoracocentesis, chest tube |
|||
|
Dulchavsky, 1988 [13] |
Pleural effusion |
N/A |
N/A |
No |
Drainage, TPN, NPO, thoracic duct ligation |
Thoracotomy |
Chest tube |
N/A |
144 |
Recovered |
|
Brook 1988 [55] |
Pleural effusion |
N/A |
N/A |
Yes |
Drainage, NPO, TPN, low-fat/ high-protein diet |
N/A |
Chest tube |
10 |
32 |
Recovered |
|
Pai, 1984 [27] |
Fracture dislocations of C6-C7 and T11-T12, right hemothorax |
N/A |
N/A |
No |
Drainage, fat-free diet, TPN, thoracic duct ligation, parietal pleurectomy |
Thoracotomy |
Chest tube |
N/A |
N/A |
Recovered |
|
Krishnan 1982 [56] |
Pleural effusion, obliteration of left costophrenic angle, multiple rib fractures |
N/A |
N/A |
No |
Drainage, thoracic duct ligation |
Thoracotomy |
Chest tube |
19 |
5 |
Recovered |
|
Azambuja 1981 [57] |
Hemopneumothorax |
N/A |
N/A |
No |
Drainage, thoracic duct ligation, pleural flap to address fistula, pleural abrasion |
Thoracotomy |
Chest tube |
6 |
N/A |
Recovered |
|
Rea 1960 [58] |
Opaque hemithorax |
N/A |
N/A |
No |
Drainage, thoracic duct ligation |
Thoracotomy |
Chest tube |
N/A |
N/A |
Recovered |
|
Guest 1955 [59] |
N/A |
N/A |
N/A |
No |
Aspiration, high-protein, low-fat diet |
N/A |
Thoracentesis |
N/A |
4 |
Recovered |
|
Elliot 1948 [60] |
Pleural effusion |
N/A |
N/A |
No |
Aspiration, thoracic duct ligation |
Thoracotomy |
Aspiration |
N/A |
N/A |
Recovered |
|
Dorsey 1942 [61] |
Rib fracture, pleural effusion |
N/A |
N/A |
No |
Drainage, low-fat diet, high-carb, high-protein diet, NPO |
N/A |
Thoracentesis |
N/A |
N/A |
Died due to uncontrolled leakage |
|
Cellan-Jones 1940 [62] |
Pleural effusion |
N/A |
N/A |
No |
Aspiration, low-fat diet, intravenous glucose-saline |
N/A |
Aspiration |
N/A |
N/A |
Died due to uncontrolled leakage |
|
Brown 1937 [63] |
Pleural effusion |
N/A |
N/A |
No |
Drainage, dietary management |
N/A |
Thoracentesis, paracentesis |
N/A |
N/A |
Died |
|
Bauersfeld 1937 [64] |
Pleural effusion, mediastinal shift |
N/A |
N/A |
No |
Drainage, intravenous dextrose, high-calorie diet |
N/A |
Thoracentesis |
16 |
N/A |
Recovered |
|
Lillie 1935 [65] |
Pleural effusion, mediastinal displacement |
N/A |
N/A |
No |
Drainage, fat-free diet |
N/A |
Thoracentesis |
N/A |
N/A |
Recovered |
|
Macnab 1932 [66] |
Displacement of the heart, pleural effusion |
N/A |
N/A |
No |
Drainage, carbohydrates, protein |
N/A |
Aspiration |
48 |
2 |
Died due to extreme asthenia |
|
CT: computed tomography, MRI: magnetic resonance imaging, ICU: intensive care unit, NPO: Nulla Per Os, TPN: total parenteral nutrition, N/A: non-available, EUS: endoscopic ultrasound |
||||||||||
Presentation and etiology
The patients ranged in age from 11 months to 84 years, with a mean of 37.4 ± 19.9 years. Most cases were male (73.91%), while females accounted for 26.09%. The most common presenting symptom or clinical findings were dyspnea, observed in 47.83% of cases, followed by abnormal findings on auscultation or percussion (34.78%) and multiple fractures or injuries (27.54%). Other frequent symptoms included chest pain (21.74%) and pneumothorax, hemothorax, or hemopneumothorax (20.29%). Road traffic accidents (RTA) were the most prevalent cause of BCTC, accounting for 59.42% of cases, followed by falls (23.19%), trauma caused by heavy objects (8.70%), physical punishment or child abuse (4.34%), and fistfights (1.45%). Bilateral chylothorax was observed in 27.54% of cases, while 55.07% had right-sided involvement and 17.39% had left-sided involvement. The chyle leakage ranged widely, which was >1000–2000 mL/day in 40.58% of cases. Smaller volumes (<500 mL/day) were noted in 14.50% and 500 – 1000 mL/day in 20.28%. In 14.50% of cases, >2000 mL/day was drained. Chyle onset occurred within two days of presentation in 40.58% of cases and within three days to a week in 31.88%. Delayed onset (beyond one week) was reported in 13.04% of cases. The chyle predominantly contained only lipids (40.57%). Other compositions included lipid-protein mixtures (11.59%) and lipid-inflammatory cells (7.24%). Complex mixtures of lipids, proteins, sugars, inflammatory cells, and ions were seen in smaller proportions (5.80%) (Table 3).
|
Variables |
Frequency / Percentage |
|
Patient demography |
|
|
Age range (mean ± SD), years |
11 months – 84 (37.4 ± 19.9) |
|
Gender Male Female |
51 (73.91%) 18 (26.09%) |
|
Common presentation and clinical findings* Dyspnea Abnormal auscultation or percussion Multiple fractures or injuries Chest pain Pneumothorax/ hemothorax/ hemopneumothorax Back pain Respiratory distress |
33 (47.83%) 24 (34.78%) 19 (27.54%) 15 (21.74%) 14 (20.29%) 11 (15.94%) 11 (15.94%) |
|
Cause of blunt trauma Road traffic accident Fall Hit or crushed by heavy objects Physical punishment & child abuse Fistfight Others |
41 (59.42%) 16 (23.19%) 6 (8.70%) 3 (4.34%) 1 (1.45%) 2 (2.90%) |
|
Side of chylothorax Right Left Bilateral |
38 (55.07%) 12 (17.39%) 19 (27.54%) |
|
Amount of chyle (ml/day) <500 500 - 1000 >1000-2000 >2000 N/A |
10 (14.50%) 14 (20.28%) 28 (40.58%) 10 (14.50%) 7 (10.14%) |
|
Chyle onset after presentation (day) At once – 2 days 3 days – one week > one week – one month > one month N/A |
28 (40.58%) 22 (31.88%) 6 (8.70%) 3 (4.34%) 10 (14.50%) |
|
Biochemical content of chyle Lipid Lipid + Protein Lipid + Inflammatory cells Lipid + Protein + Sugar + Inflammatory cells + Ions Lipid + Protein + Sugar Lipid + Inflammatory cells + Protein N/A |
28 (40.57%) 8 (11.59%) 5 (7.24%) 4 (5.80%) 2 (2.90%) 2 (2.90%) 20 (29.00%) |
|
Imaging findings |
|
|
Chest X-rays* Pleural effusion Rib Fracture Lung/ mediastinal/ heart shift Opacification of lung Pneumothorax/ hemothorax Lung contusion Pneumomediastinum Vertebral fracture Lung consolidation Others N/A |
38 (55.07%) 7 (10.14%) 7 (10.14%) 6 (8.70%) 5 (7.24%) 2 (2.90%) 1 (1.45%) 1 (1.45%) 1 (1.45%) 5 (7.24%) 15 (21.74%) |
|
CT scan findings* Pleural effusion Rib fracture Vertebral fracture Pneumothorax/ hemothorax/ hemopneumothorax Lung contusion Pneumomediastinum Hematoma Thoracic duct leakage Others N/A |
23 (33.33%) 14 (20.29%) 10 (14.50%) 9 (13.04%) 8 (11.59%) 4 (5.80%) 3 (4.34%) 2 (2.90%) 17 (24.64%) 25 (36.23%) |
|
ICU admission Yes No |
19 (27.54%) 50 (72.46%) |
|
Common treatment approach* Drainage Parenteral nutrition Thoracic duct ligation/embolization/suturing Medium-chain fatty acid or low-fat diet Nulla per Os Free fat diet/starvation diet Octreotide Pleurectomy/Pleurodesis |
65 (94.20%) 35 (50.72%) 27 (39.13%) 24 (34.78%) 19 (27.54%) 12 (17.39%) 17 (24.64%) 6 (8.70%) |
|
Thoracic duct closure approach Thoracotomy Fr microcatheter with fluoroscopic/ ultrasound guidance VATS/ laparoscopy Coiling and glue embolization Unknown Not performed |
22 (31.88%) 2 (2.90%) 2 (2.90%) 1 (1.45%) 1 (1.45%) 41 (59.42%) |
|
Mode of drainage Chest tube Thoracentesis Aspiration Chest tube + Thoracentesis |
53 (76.81%) 9 (13.04%) 4 (5.80%) 3 (4.34%) |
|
Duration of chest tube placement ≤ One week > One week – two weeks > Two weeks – one month > One month N/A |
12 (17.39%) 11 (15.94%) 13 (18.84%) 4 (5.80%) 29 (42.03%) |
|
Outcome Recovered Partially recovered Died |
62 (89.85%) 1 (1.45%) 6 (8.70%) |
|
SD: standard deviation, CT: computed tomography, ICU: intensive care unit, VATS: video-assisted thoracoscopic surgery, N/A: non-available. *Each data in the variable might be found in more than one case |
|
Imaging characteristics and management
Chest X-rays revealed pleural effusion in 55.07% of cases, rib fractures, and lung or mediastinal or heart shift, each in 10.14%, lung opacification in 8.70%, and pneumothorax or hemothorax in 7.24%. Computed tomography (CT) scans confirmed pleural effusion in 33.33% and rib fractures in 20.29%. The vertebral fracture was found in 14.50%, and pneumothorax, hemothorax, or hemopneumothorax in 13.04%. Drainage was performed in 94.20%, predominantly via chest tubes (76.81%). In 17.39% of patients, the chest tube was in place for one week or less, while 15.94% required chest tube placement for more than one week until two weeks. Another 18.84% needed chest tube placement for over two weeks to one month, and 5.80% had chest tube placement exceeding one month. Additional treatments included parenteral nutrition (50.72%), thoracic duct closure (39.13%), and dietary modifications such as a medium-chain fatty acid or low-fat diet (34.78%). Pharmacological treatments included octreotide in 24.64% of cases. Thoracic duct closure was performed through thoracotomy in 31.88%. Other less-used techniques included Fr microcatheter under radiological guidance in 2.90%, video-assisted thoracoscopy or laparoscopy in 2.90%, and coiling and glue embolization in 1.45%. In 59.42% of cases, thoracic duct closure was not performed. The majority of patients (89.85%) achieved complete recovery, with one case showing partial recovery (1.45%), and six cases died (8.70%) (Table 3).
Discussion
Chylothorax is a pathological condition; if left untreated, it can result in respiratory distress and various complications. The etiology is multifaceted, including traumatic causes, while non-traumatic factors may involve conditions that elevate lymphatic pressure or cause obstruction, such as lymphoma or heart failure [1,67]. Chylothorax was first documented in the medical literature during the 19th century but has since garnered increasing recognition with advancements in diagnostic and surgical techniques. Improved imaging modalities and surgical innovations have significantly enhanced the understanding of its pathophysiology, facilitating more effective identification and management of its underlying causes [1,2].
The demographic data in the present review revealed an age range of 11 months to 84 years, with a mean age of 37.4 ± 19.9 years. This aligns with the literature, as Elsaied et al. reported an approximate mean age of 42.67 years within an age range of 18 to 76 years [68]. Case reports have identified young adults as particularly susceptible to chylothorax following blunt chest trauma, who are commonly involved in motor vehicle collisions or sports injuries [12,31]. Conversely, another study found that individuals aged 50 years or older represented the most common age group among blunt chest trauma patients, comprising 28.9% of the sample [69]. This reflects the increased risk of falls and accidents among older populations [70]. The slightly lower mean age in the present study may be attributable to the inclusion of pediatric cases, broadening the demographic scope. A significant male predominance was observed in the current review, with 73.91% of cases involving males. This finding concurs with the literature, where male representation ranged from 72.3% in a literature review [71] to 85.4% in a cohort study on blunt chest trauma cases [69]. This gender disparity is often linked to higher exposure to high-risk activities and occupations among males [12,31].
The clinical presentation of chylothorax is variable, with dyspnea being the most common symptom, reported by approximately 66.7% of patients. Dyspnea arises from fluid accumulation in the pleural space, which restricts lung expansion and impairs gas exchange. Patients may also experience a dry cough, often exacerbated by pleural fluid [72]. Pleuritic chest pain is another potential symptom, likely caused by pleural irritation from chyle [3,5]. On physical examination, percussion of the thorax often reveals dullness over the affected area due to fluid accumulation, contrasting with the typical resonance of healthy lung tissue [3,12,22]. Auscultation typically shows diminished or absent breath sounds over regions where fluid has accumulated, reflecting impaired air movement [72]. In this review, consistent with the literature, dyspnea was the most common presenting symptom (47.83%). This was followed by abnormal findings on auscultation or percussion in 34.78% of cases. Other frequently reported symptoms included chest pain (21.74%) and complications such as pneumothorax, hemothorax, or hemopneumothorax (20.29%).
The thoracic duct, the primary conduit for lymphatic fluid, can be ruptured or injured by blunt trauma, leading to chyle leakage into the pleural space [71,73]. Damage to adjacent structures, such as vertebral fractures or mediastinal injuries, can also contribute to chylothorax. For example, thoracic spine injuries have been associated with chylothorax due to their anatomical proximity to the thoracic duct [4,14]. Chylothorax is predominantly unilateral. In a study of 74 cases, 78% involved one hemithorax, with the right side being affected in 67% and the left in 33%. Bilateral pleural effusion was observed in 22% of cases [74]. The volume of chyle leakage varies based on the severity of the injury and the extent of thoracic duct damage. Low-output chylothorax (<1000 mL/day) is typically managed conservatively, whereas high-output cases (>1–1.5 L/day) often require surgical or radiological intervention [4,37,75]. In extreme cases, chyle output exceeding 2000 mL/day has been reported [6,15,21,30]. Blunt chest trauma frequently results from RTA, underscoring the risks of high-speed collisions [5,22,32]. Falls are another common cause, accounting for approximately 45% of cases in a study of patients with multiple traumas [76]. In this review, RTA was found to be the leading cause of injury in 41 cases (59.42%), followed by falls in 16 cases (23.19%), trauma by heavy objects in 6 cases (8.70%), physical punishment or child abuse in three cases (4.34%) and fistfights in one case (1.45%). Bilateral chylothorax occurred in 27.54% of cases, higher than previously reported. Consistent with the literature, right-sided involvement (55.07%) was more common than left-sided involvement (17.39%). This finding contrasts with the observation of Kakamad et al., who reported no laterality difference, but is similar to the findings of Maldonado et al., who reported right-sided involvement in 67% of cases and left-sided involvement in 33% [71,74]. Chyle volume varied significantly, with 40.58% of cases producing >1000–2000 mL/day, while 10 cases (14.50%) exceeded 2000 mL/day.
The timing of chyle onset in this review varied, with symptoms developing within two days in 40.58% of cases and within three days to a week in 31.88%. These align with the finding that chylothorax most commonly manifests within 2 to 7 days following blunt chest trauma due to gradual pleural accumulation from duct leakage [71]. However, delayed onset beyond one month, as observed in 4.34% of reviewed cases, is rare but documented in the literature, with an extreme case reported up to 20 years post-trauma [18]. The biochemical composition of chyle among the reviewed cases primarily consisted of lipids (40.57%), with smaller proportions of lipid-protein mixtures (11.59%) and lipid-inflammatory cell mixtures (7.24%). Complex mixtures, including lipids, proteins, sugars, inflammatory cells, and ions, were identified in 5.80% of cases. These findings are consistent with the established biochemical profile of chyle, which is rich in triglycerides (≥110 mg/dL) and lymphocytes [71]. As reported in the literature, immunoglobulins and protein levels ranging from 2.2 to 6 g/dL underscore the nutritional and immunological impact of chyle loss [1,8,32].
In the present review, chest X-rays revealed pleural effusion in 55.07% of cases, consistent with its status as the most common radiographic finding in chylothorax, typically presenting as a homogeneous opacity [2,4,32,71]. Rib fractures and lung or mediastinal or heart shift each were observed in 10.14% of cases, with lung opacification in 8.70% and pneumothorax, or hemothorax in 7.24%, aligning with literature that highlights the utility of chest X-rays in detecting associated traumatic injuries, such as rib fractures and pulmonary contusions [2,6,77]. CT scans in the reviewed cases showed pleural effusion in 33.33% of cases and rib fractures in 20.29%. The detection of pneumothorax, hemothorax, or hemopneumothorax in 13.04% of cases further emphasizes the role of CT in visualizing coexisting traumatic injuries with greater detail than X-rays [4,77].
The initial approach to managing chylothorax primarily involves conservative measures, including nil per os (nothing by mouth), total parenteral nutrition, and adherence to a low-fat diet. Pharmacological interventions, such as octreotide, may decrease lymphatic flow and facilitate the closure of the leak [10,14,21,23]. In chylothorax management, chest tube placement is commonly maintained until chyle drainage significantly decreases or resolves. The duration varies from a few days to several weeks, influenced by the effectiveness of conservative approaches [78]. In this review, the chest tube was in place for one week or less in 17.39% of patients, while 15.94% required chest tube placement for more than one week until two weeks. Another 18.84% needed chest tube placement for over two weeks to one month, and 5.80% had chest tube placement exceeding one month.
In cases where conservative management proves ineffective, surgical intervention becomes imperative. Thoracic duct ligation remains the definitive surgical option and can be performed via open thoracotomy or minimally invasive approaches [79]. Based on the findings of this review, besides drainage, treatments for chylothorax included parenteral nutrition (50.72%), thoracic duct closure (39.13%), and dietary modifications, such as a medium-chain fatty acid or low-fat diet (34.78%). Octreotide was administered in 24.64% of cases. Thoracic duct closure was performed via thoracotomy in 31.88% of cases, Fr microcatheter with fluoroscopic/ ultrasound guidance in 2.90%, VATS or laparoscopy in 2.90%, and coiling and glue embolization in 1.45%. In 59.42% of cases, thoracic duct closure was not performed or was unnecessary.
The limitations of this study include the inherent nature of the reviewed studies, which were exclusively case reports due to the rarity of the condition. Consequently, drawing conclusions based on statistical analyses was not feasible. Additionally, the small sample size and the non-standardized data reporting across the included reports may have introduced potential bias into the findings of this review. While every effort was made to include all relevant studies identified through the search using predefined keywords, there remains the possibility that some studies were inadvertently overlooked.
Conclusion
BCTC is rare and complex, underscored by the wide variability in patient demographics, clinical presentations, chylothorax onset, and management approaches. Given the challenges posed by limited evidence, the findings emphasize the need for early recognition and individualized management strategies.
Declarations
Conflicts of interest: The authors have no conflicts of interest to disclose.
Ethical approval: Not applicable.
Consent for participation: Not applicable.
Consent for publication: Not applicable.
Funding: The present study received no financial support.
Acknowledgements: None to be declared.
Authors' contributions: FHK and HOA: major contributors to the conception of the study, as well as the literature search for related studies, and manuscript writing. HKA, BJHA, and HMA: Literature review, critical revision of the manuscript, and processing of the tables. SHM, BeAA, SMA, MNH, SSA, YMM, KAN, SHK and BaAA: Data extraction, data organization, and critical revision. All authors have read and approved the final version of the manuscript.
Use of AI: ChatGPT-3.5 was used to assist with language refinement and improve the overall clarity of the manuscript. All content was thoroughly reviewed and approved by the authors, who bear full responsibility for the final version.
Data availability statement: Not applicable.
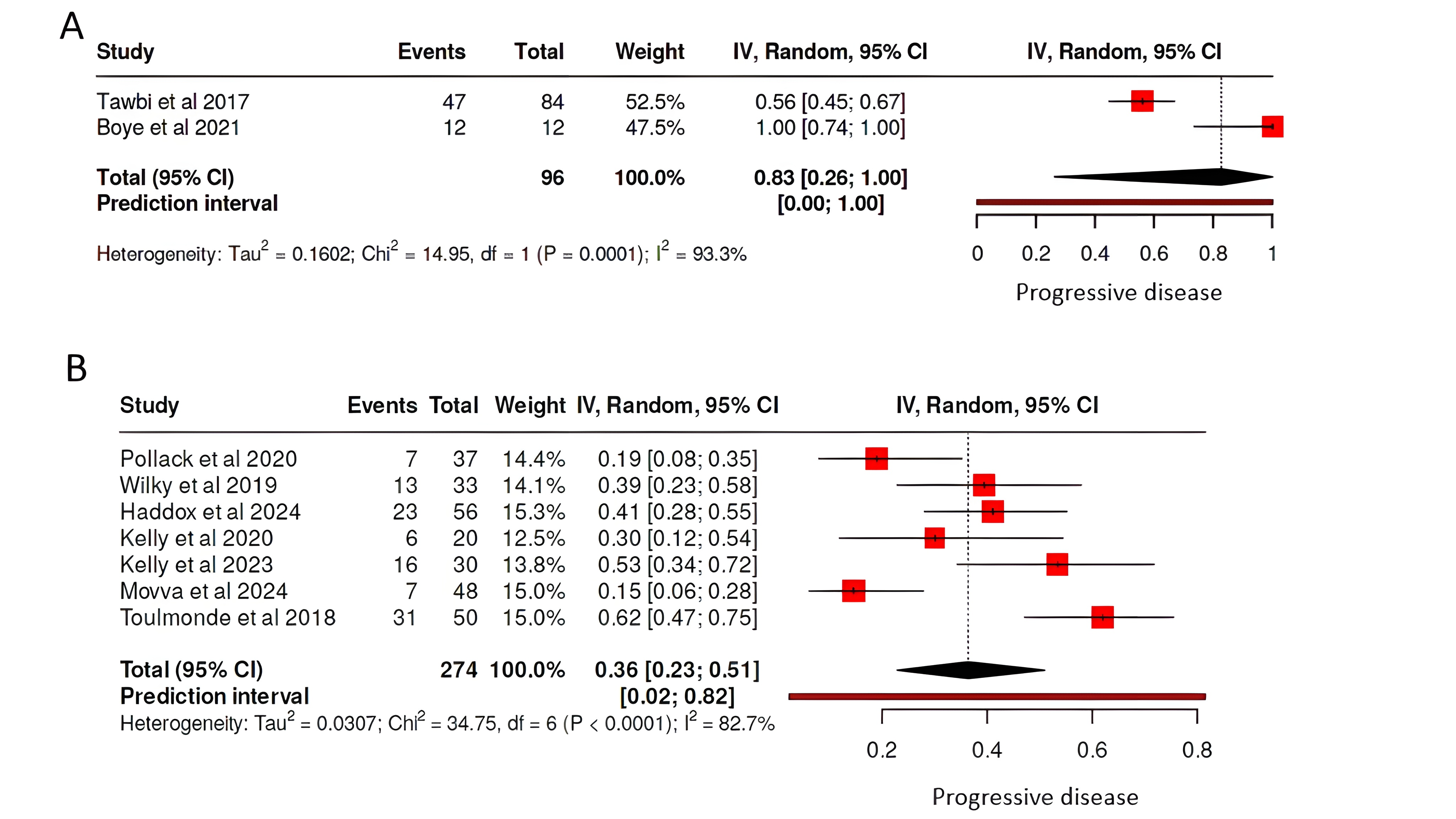
Pembrolizumab and Sarcoma: A meta-analysis
Rebaz M. Ali, Sami S. Omar, Shalaw H. Abdalla, Fattah H. Fattah, Shnya R. Hamalaw, Hussein M....
Abstract
Introduction: Pembrolizumab is a monoclonal antibody that promotes antitumor immunity. This study presents a systematic review and meta-analysis of the efficacy and safety profile of this treatment as monotherapy or in combination with other drugs for the treatment of sarcomas.
Methods: A literature search was conducted across Google Scholar, PubMed/MEDLINE, and EMBASE from February 15th to April 15th. Eligible studies were clinical trials that reported efficacy or outcomes of pembrolizumab in sarcoma patients, either alone or in combination with other drugs. In contrast, those lacking sufficient data or not meeting trial criteria were excluded.
Results: Ten clinical trials met the eligibility criteria, including 419 sarcoma patients (53.7% male; median age 55.4). Pembrolizumab was administered either as monotherapy in 23% of cases or in combination with other agents in 77% of cases. The progressive disease rate was 83% with monotherapy and 36% with combination therapy. Objective response rates varied, with the highest observed in the pembrolizumab plus talimogene laherparepvec combination (35%) and the lowest in pembrolizumab monotherapy (ranging from 0% to 11.2%). Median progression-free survival ranged from 1.4 (Pembrolizumab + Cyclophosphamide) to 7.8 months (Pembrolizumab + Lenvatinib in undifferentiated pleomorphic sarcoma). Combination therapy was associated with significantly better tumor response (<0.001). However, rates of endocrine, gastrointestinal, some hepatic, and dermatological adverse events were significantly associated with combination therapy compared to monotherapy (p < 0.05).
Conclusion: Pembrolizumab-based combination therapies have the potential to enhance treatment efficacy in sarcoma, although they may be associated with an increased risk of adverse events.
Introduction
Sarcomas are rare tumors that develop from mesenchymal tissue and are known for their diverse histological subtypes. Although they are uncommon, they carry particular clinical significance due to their relatively higher incidence in adolescents and young adults. The primary treatment is surgical resection, often combined with chemotherapy or radiotherapy, either before (neoadjuvant) or after (adjuvant) surgery, depending on the specific subtype [1].
Immunotherapy has introduced a breakthrough in cancer treatment. Unlike traditional approaches such as chemotherapy and radiation, which can harm healthy cells and lead to significant side effects, immunotherapy takes a more targeted and refined approach. It helps the body’s immune system recognize and attack cancer cells, offering a potentially more effective and less toxic alternative [2].
Cancer immunotherapy includes a variety of treatment methods, such as immune checkpoint inhibitors, adoptive cell transfer, cytokine therapies, and cancer vaccines [3]. What sets immunotherapy apart is its ability to produce long-lasting effects, sometimes leading to extended remission or even complete disappearance of the disease in some patients [4]. In addition, immunotherapy is often better tolerated than traditional treatments, since it tends to focus more precisely on cancer cells while causing less harm to healthy tissues [2].
Pembrolizumab is a monoclonal antibody that targets the programmed cell death protein 1 (PD-1) receptor, blocking its interaction with the ligands PD-L1 and PD-L2, which are often expressed by tumor cells. By interrupting this pathway, pembrolizumab removes a key mechanism of immune suppression, allowing cytotoxic T cells to become more active and better able to attack cancer cells [5]. PD-1 is an immune checkpoint receptor found on activated T cells. When it binds to PD-L1 or PD-L2, it downregulates immune activity by inhibiting T-cell function and helping tumor cells avoid destruction. Research has shown that tumors often increase PD-L1 expression as a strategy to escape immune detection, weakening the body’s ability to fight cancer [6].
Despite significant research, sarcomas remain difficult to treat effectively. Soft tissue sarcomas, in particular, have a 5-year survival rate of only about 65%, highlighting the ongoing need for more effective therapeutic options [1]. Pembrolizumab has shown durable antitumor activity across several solid tumor types, along with a generally favorable safety and tolerability profile [7]. This systematic review and meta-analysis aims to assess the antitumor efficacy and safety of pembrolizumab, both as a standalone therapy and in combination with other agents, in treating different types of sarcomas through a systematic review and meta-analysis of clinical trials. Only data from peer-reviewed sources were included, ensuring the reliability of the data [8].
Methods
Study design
The study is a systematic review and meta-analysis encompassing clinical trials assessing the effectiveness of pembrolizumab in treating sarcomas. It encompasses trials where pembrolizumab is used alone as well as in combination with other treatments. The drug combinations were as follows: group A (Pembrolizumab + Doxorubicin), group B (Pembrolizumab + Axitinib), group C (Pembrolizumab + Eribulin), group D (Pembrolizumab + Talimogene Laherparepvec), group E (Pembrolizumab + Epacadostat), group F (Pembrolizumab + Olaratumab), group G (Pembrolizumab + Levatinib), and group H (Pembrolizumab + Cyclophosphamide). The search process was conducted from February 15th to April 15th 2025, in full compliance with the PRISMA 2020 (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines.
Data sources and search strategy
A thorough search was performed using Google Scholar, PubMed/MEDLINE, and EMBASE. A set of keywords was utilized to retrieve pertinent studies, specifically: (anti-PD-1; PD-1 inhibitor; Keytruda; MK-3475; Lambrolizumab; Pembrolizumab; Sarcoma; Sarcomas; Spindle cell sarcoma; Spindle cell sarcomas).
Eligibility criteria
Eligible studies consisted of clinical trials evaluating the efficacy of pembrolizumab in treating sarcomas, either as a standalone therapy or in combination with other treatments. Studies were excluded if they were not clinical trials, did not investigate pembrolizumab for sarcoma treatment, or failed to provide adequate data on treatment efficacy or patient outcomes.
Study selection process
The study selection process was conducted independently by two researchers who carefully screened the titles and abstracts of all identified studies. Each study was assessed based on the predefined inclusion and exclusion criteria. In instances of disagreement regarding a study’s eligibility, a third researcher was consulted to resolve the conflict and reach a consensus.
Data items
Data extracted from the eligible studies encompassed a wide range of information, including the first author’s name, year of publication, trial phase, sarcoma subtype, number of enrolled patients, sex distribution, treatment regimen, median patient age, reported adverse events, and various clinical outcome measures, including progression-free survival, overall survival, complete response, partial response, stable disease and progressive disease.
Data analysis and synthesis
The extracted data were organized using Microsoft Excel (2019) and analyzed with SPSS version 25.0 (IBM Corp.). Descriptive statistics were reported as frequencies, percentages, medians, and ranges. Categorical variables were compared using the Chi-square or Fisher's exact test, as appropriate. Continuous variables, including overall survival and progression-free survival (PFS), were analyzed using the non-parametric Mann-Whitney U test.
Results
Study selection process and eligibility criteria
A total of 103 records were initially identified through the search process. Among these, 42 were excluded because they were unretrievable, two were removed as duplicates, and one was excluded for not qualifying as a full research article. Then, the titles and abstracts of the remaining 58 studies were screened, resulting in the exclusion of 20 records that were deemed irrelevant. After that, 38 studies underwent full-text screening, of which 27 were excluded based on exclusion criteria. Subsequently, 11 studies were assessed for eligibility, and one was excluded because it did not provide complete data. In the end, 10 studies were included for final review and analysis (Figure 1) [7, 9-17].
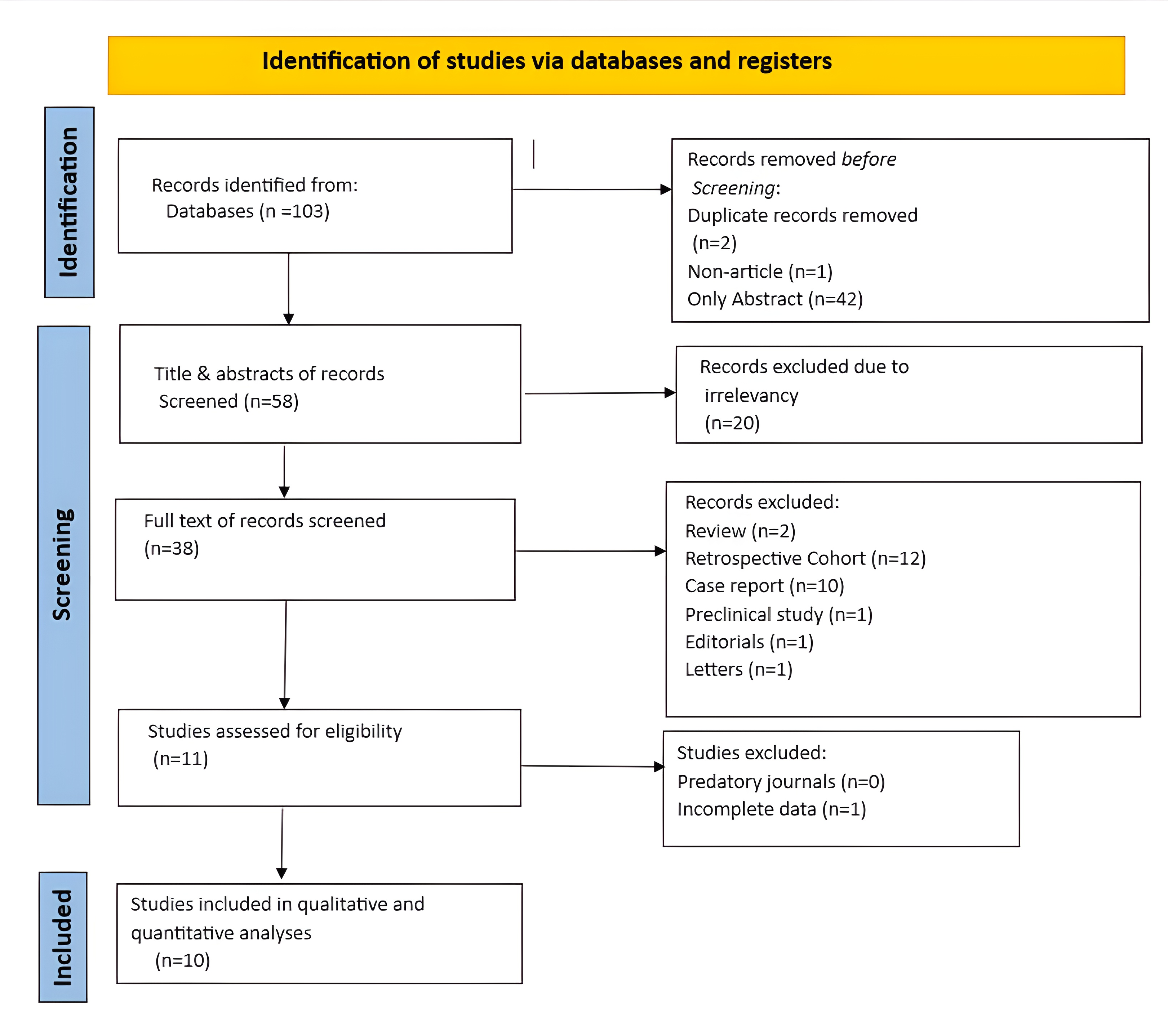
Characteristics of included trials
All the studies included were clinical trials, consisting of eight Phase II trials, one Phase I trial, and one study that encompassed both Phase I and II designs. The raw data, along with key characteristics of each study, are summarized in Tables 1, 2, and 3. Analysis of progressive disease rates in sarcoma patients treated with pembrolizumab monotherapy, based on two studies, revealed an overall rate of 83% (95% CI: 26%–100%). In contrast, a meta-analysis of patients receiving pembrolizumab in combination with other therapeutic agents showed a substantially lower progressive disease rate of 36% (95% CI: 23%–51%) (Figure 2).
![Figure 2. Forest plot of studies evaluating progressive disease rates with (A) Pembrolizumab monotherapy vs. (B) Pembrolizumab combination therapies*. CI, confidence interval *Olaratumab combination trial was excluded due to unavailable progressive disease data [16].](https://www.judijournal.com/public/site/images/journaleditor/mceu-5288121221751108819164.png)
|
First Author /Year [reference] |
Trial Phase |
Type of sarcoma |
Therapy regimens
|
No. of patients |
Sex |
Median Age |
|
|
Male |
Female |
||||||
|
Pollack et al,2020 [10] |
I/II |
Soft tissue sarcoma |
Pembrolizumab 200mg/q3w(IV) Doxorubicin 45-75mg |
37 |
22 |
15 |
58.4 |
|
Wilky et al, 2019 [11] |
II |
Soft tissue sarcoma |
Pembrolizumab 200mg/q3w (IV) Axitinib 5mg (Orally) |
33 |
18 |
15 |
44 |
|
Tawbi et al,2017 [9] |
II |
Soft tissue sarcoma + Osteosarcoma |
Pembrolizumab 200mg/q3w (IV) |
84 |
53 |
31 |
53a/ 33b |
|
Haddox et al,2024 [17] |
II |
Soft tissue sarcoma |
Pembrolizumab 200mg/q3w(IV) Eribulin 1.4mg/m2 (iv) |
57 |
24 |
33 |
60.4* |
|
Kelly et al,2020 [13] |
II |
Soft tissue sarcoma |
Pembrolizumab 200mg/q3w(IV) Talimogene Laherparepvec ≤4ml×102 (intratumourally) |
20 |
12 |
8 |
58.3 |
|
Kelly et al, 2023 [14] |
II |
Soft tissue sarcoma |
Pembrolizumab 200mg/q3w (IV) Epacadostat 100mg (orally) |
30 |
18 |
12 |
54 |
|
Schöffski et al, 2023 [16] |
Ia/b |
Soft tissue sarcoma |
Pembrolizumab 200mg/q3w(IV) Olaratumab 15-20mg/kg (IV) |
41 |
15 |
26 |
56.83* |
|
Movva et al,2024 [12] |
II |
Soft tissue sarcoma + Bone sarcoma |
Pembrolizumab 200mg/q3w(IV) Levatinib 20mg (orally) |
48 |
22 |
26 |
50 |
|
Toulmonde et al, 2018 [15] |
II |
Soft tissue sarcoma |
Pembrolizumab 200mg/q3w (IV) Cyclophosphamide 50mg (Orally) |
57 |
33 |
24 |
59.5 |
|
Boye et al,2021 [7] |
II |
Osteosarcoma |
Pembrolizumab 200mg/q3w (IV) |
12 |
8 |
4 |
43 |
|
*: mean age, a: median age in soft tissue sarcoma, b: median age in bone sarcoma, q3w: every three weeks, IV: intravenous |
|||||||
|
First Author /Year [reference] |
Patient No. (Evaluable for response) |
Prior chemotherapy |
Therapy Regimen |
Outcome |
ORR (%) |
|||||||
|
Yes |
No |
CR |
PR |
SD |
PD |
NE |
||||||
|
Pollack et al,2020 [10] |
37 |
9 |
28 |
Group A |
0 |
7 |
22 |
7 |
1 |
|
||
|
Wilky et al, 2019 [11] |
30 |
27 |
6 |
Group B |
0 |
8 |
9 |
13 |
3 |
|
||
|
Tawbi et al,2017 [9] |
80 |
80 |
0 |
Pembrolizumab alone |
1 |
8 |
24 |
47 |
4 |
11.2
|
||
|
Haddox et al,2024 [17] |
56 |
2.5(1.5)a |
0 |
Group C |
1b |
10
|
22 |
23 |
1 |
19.3
|
||
|
Kelly et al,2020 [13] |
20 |
19 |
1 |
Group D |
0 |
7 |
7 |
6 |
0 |
35
|
||
|
Kelly et al, 2023 [14] |
30 |
24 |
6 |
Group E |
0 |
1 |
13 |
16 |
0 |
3.3
|
||
|
Schöffski et al, 2023 [16] |
41 |
37 |
0 |
Group F |
0 |
6 |
N/A |
N/A |
N/A |
14.6
|
||
|
Movva et al,2024 [12] |
46 |
43 |
5 |
Group G |
0 |
8 |
31 |
7 |
2 |
15.2
|
||
|
Toulmonde et al, 2018 [15] |
48 |
55 |
2 |
Group H |
0 |
1 |
16 |
31 |
9 |
2
|
||
|
Boye et al,2021 [7] |
12 |
12 |
0 |
Pembrolizumab alone |
0 |
0 |
0 |
12 |
0 |
0
|
||
|
RECIST: Response Evaluation Criteria in Solid Tumors, ORR: Objective response rate, CR: complete response, PR: Partial response, SD: Stable disease, PD: progressive disease, NE: not evaluable. (a): mean (SD), (b) The patient had radiotherapy-associated angiosarcoma. |
||||||||||||
|
First Author /Year [reference] |
Patient No. |
Therapy Regimen |
RMD (months) |
Median follow-up (months) |
Median PFS (months) |
Median Overall survival (months) |
|
Pollack et al, 2020 [10] |
37 |
Group A |
N/A |
N/A |
8.1 |
27.6 |
|
Wilky et al, 2019 [11] |
33 |
Group B |
6.6 |
14.7 |
4.7 |
18.7 |
|
Tawbi et al, 2017 [9] |
84 |
Pembrolizumab alone |
7.6a/9.9b |
19.1a/17.8b |
4a/2b |
11.2a/12b |
|
Haddox et al, 2024 [17] |
57 |
Group C |
N/A |
14c/11.6d/7e |
2.5c/7.3d/2.9e
|
13.5c/22d/N/Ae |
|
Kelly et al, 2020 [13] |
20 |
Group D |
13 |
13 |
4 |
N/A |
|
Kelly et al, 2023 [14] |
30 |
Group E |
N/A |
29.7 |
1.7 |
16.9 |
|
Schöffski et al, 2023 [16] |
41 |
Group F |
16.2 |
N/A |
1.4f/2.8g/2.7h |
11.4f/16.4g/14.8h |
|
Movva et al, 2024 [12] |
48 |
Group G |
2.5 |
20 |
2.2c/5.7A/7.8B/6.4C/4.3D |
10.3A/N/AB/14.5C/13.8D/6.4E |
|
Toulmonde et al, 2018 [15] |
57 |
Group H |
N/A |
6.8 |
1.4 |
9.2 |
|
Boye et al, 2021 [7] |
12 |
Pemb. alone |
N/A |
N/A |
1.7 |
6.6 |
|
RMD: response median duration, PFS: progression-free survival, a: soft tissue sarcoma, b: bone sarcoma, c: Leiomyosarcoma, d: Liposarcoma, e: Undifferentiated pleomorphic sarcoma/other, f: Olaratumab plus Pembrolizumab, g: Olaratumab plus Pembrolizumab, h: Olaratumab Pembrolizumab, A: undifferentiated pleomorphic sarcoma, B: vascular sarcomas (angiosarcoma and epithelioid hemangioendothelioma), C: synovial sarcoma or malignant peripheral nerve sheath tumor, D: bone sarcomas (osteosarcoma and chondrosarcoma). |
||||||
Baseline characteristics and treatment group distribution
A total of 419 patients were included across the eligible studies, of which 225 (53.7%) were males. The median age (IQR) of the patients was 55.4 (14.4). Most patients had an Eastern Cooperative Oncology Group (ECOG) status of zero (156, 37.23%), followed by a score of one (139, 33.17%). Performance status was not reported for 124 patients (29.6%). Histologically, leiomyosarcoma was the most frequently reported subtype, accounting for 99 cases (25.85%), whereas conventional chondrosarcoma was the least common, identified in only three cases (0.78%). Three hundred twenty-nine (78.52%) patients exhibited both metastatic and locally advanced properties. Patients were categorized into two groups: 96 patients (23%) received pembrolizumab as a monotherapy, while 323 patients (77%) were treated with pembrolizumab in combination with other therapies. The types of sarcoma included in the trials were soft tissue sarcoma (354, 84.5%) and bone sarcoma (65, 15.5%) (Table 4).
|
Variables |
Frequency/percentage |
|
Median age (IQR) |
55.4 (14.4) |
|
Sex Male Female |
225 (53.7%) 194 (46.3%) |
|
ECOG Status ECOG status (0) ECOG status (1) Not mentioned |
156 (37.23%) 139 (33.17%) 124 (29.6%) |
|
Sarcoma types Soft tissue sarcoma Bone sarcoma |
354 (84.5%) 65 (15.5%) |
|
Histological subtypes Angiosarcoma Synovial sarcoma Dedifferentiated liposarcoma Pleomorphic liposarcoma Leiomyosarcoma Undifferentiated pleomorphic sarcoma Gastrointestinal stromal tumor Alveolar soft-part sarcoma Osteosarcoma Dedifferentiated chondrosarcoma Ewing sarcoma Conventional chondrosarcoma Others |
Evaluable patients (383) 17 (4.44%) 22 (5.74%) 40 (10.44%) 4 (1.04%) 99 (25.85%) 63 (16.45%) 11 (2.87%) 13 (3.39%) 36 (9.4%) 10 (2.61%) 15 (3.92%) 3 (0.79%) 50 (13.05%) |
|
Sarcoma stage Locally advanced Metastatic Both |
11 (2.63%) 79 (18.85%) 329 (78.52%) |
|
Treatment group Pembrolizumab alone Pembrolizumab combination |
96 (23.0%) 323 (77.0%) |
Objective response rate (ORR) was 19% for patients treated with pembrolizumab plus doxorubicin, 25% for pembrolizumab plus axitinib, and 11.2% for pembrolizumab alone in a cohort of 80 patients. Pembrolizumab plus eribulin yielded an ORR of 19.3%, while the combination with talimogene laherparepvec had the highest ORR at 35%. In contrast, pembrolizumab plus epacadostat showed a low ORR of 3.3%, and pembrolizumab plus olaratumab achieved an ORR of 14.6% (Table 2).
Response median duration was available for five trials and ranged from 6.6 to 13 months. Median progression-free survival ranged from 1.4 months to 7.8 months, and median overall survival ranged from 6.6 to 27.6 months (Table 3).
Efficacy and adverse events in different treatment groups
Anemia affected 30% of patients overall. It was persistent with Group C (52.6%) and Group D (30%). Lymphopenia was notable in pembrolizumab monotherapy (27%). Vomiting and diarrhea were most frequent with Group B (66.6%) and (57.5%), respectively. Hypothyroidism was high in Group B (63.6%) and Group G (29.1%). Elevated liver enzymes (ALP, AST, ALT) were widespread, especially with Group G (89.5%) and Group A (59.3%). Cough and dyspnea were seen across most regimens, but cough was particularly high with Group B (33%). Headache was a relatively common complaint, notably with Group F (24.3%). Cardiac events were rare, but hypertension was notable in Group B (48.4%) and Group G (56%). Alopecia was most common in Group A (42.4%) and Group C (24.5%). Fatigue was the most common general adverse event, affecting more than half of all patients and reaching up to 80% in Group D (Table 5).
|
Adverse events |
Total (%)* |
Pemb. (96)** |
G. A (37) |
G. B (33) |
G. C (57) |
G. D (20) |
G. E (30) |
G. F (41) |
G. G (48) |
G. H (57) |
|
Hematological |
|
|
|
|
|
|
|
|
|
|
|
Thrombocytopenia |
19 (4.5%) |
0 (0.0%) |
0 (0.0%) |
0 (0.0%) |
0 (0.0%) |
1 (5%) |
1 (3.3%) |
0 (0.0%) |
17 (35.4%) |
0 (0.0%) |
|
Lymphopenia |
36 (8.6%) |
26 (27.0%) |
2 (5.4%) |
0 (0.0%) |
3 (5.2%) |
0 (0.0%) |
0 (0.0%) |
0 (0.0%) |
0 (0.0%) |
5 (8.7%) |
|
Febrile neutropenia |
13 (3.1%) |
4 (4.1%) |
3 (8.1%) |
0 (0.0%) |
6 (10.5%) |
0 (0.0%) |
0 (0.0%) |
0 (0.0%) |
0 (0.0%) |
0 (0.0%) |
|
Anemia |
126 (30.0%) |
43 (10.2%) |
5 (13.5%) |
0 (0.0%) |
30 (52.6%) |
6 (30%) |
6 (20%) |
11 (26.8%) |
13 (27%) |
12 (21%) |
|
Gastrointestinal |
|
|
|
|
|
|
|
|
|
|
|
Nausea |
138 (33.0%) |
22 (23.0%) |
32 (86.4%) |
22 (3.0%) |
25 (43.8%) |
6 (30%) |
4 (13.3%) |
6 (14.6%) |
15 (31.2%) |
6 (10.5%) |
|
Vomiting |
56 (13.4%) |
11 (11.4%) |
11 (29.7%) |
22 (66.6%) |
6 (10.5%) |
4 (20%) |
2 (6.6%) |
0 (0.0%) |
0 (0.0%) |
0 (0.0%) |
|
Anorexia |
72 (17.2%) |
14 (14.5%) |
18 (48.6%) |
12 (36.3%) |
24 (42.1%) |
0 (0.0%) |
4 (13.3%) |
0 (0.0%) |
0 (0.0%) |
0 (0.0%) |
|
Constipation |
55 (13.1%) |
17 (17.7%) |
5 (13.5%) |
9 (27.2%) |
15 (26.3%) |
0 (0.0%) |
0 (0.0%) |
9 (22%) |
0 (0.0%) |
0 (0.0%) |
|
Diarrhea |
96 (23.0%) |
15 (15.6%) |
8 (21.6%) |
19 (57.5%) |
12 (21.0%) |
0 (0.0%) |
2 (6.6%) |
12 (29.2%) |
21 (4.16) |
7 (12.2%) |
|
Decreased appetite |
7 (1.7%) |
0 (0.0%) |
0 (0.0%) |
0 (0.0%) |
0 (0.0%) |
0 (0.0%) |
0 (0.0%) |
7 (17.1%) |
0 (0.0%) |
0 (0.0%) |
|
Xerostomia |
26 (6.2%) |
0 (0.0%) |
11 (29.7%) |
0 (0.0%) |
8 (14.0%) |
0 (0.0%) |
4 (13.3%) |
0 (0.0%) |
0 (0.0%) |
3 (5.2%) |
|
Abdominal pain |
27 (6.4%) |
13 (13.5%) |
2 (5.4%) |
0 (0.0%) |
3 (5.2%) |
0 (0.0%) |
1 (3.3%) |
8 (19.5%) |
0 (0.0%) |
0 (0.0%) |
|
Colitis |
5 (1.2%) |
0 (0.0%) |
0 (0.0%) |
0 (0.0%) |
3(5.2%) |
0 (0.0%) |
0 (0.0%) |
0 (0.0%) |
2 (4.2%) |
0 (0.0%) |
|
Colonic perforation |
1 (0.2%) |
0 (0.0%) |
0 (0.0%) |
0 (0.0%) |
0 (0.0%) |
0 (0.0%) |
0 (0.0%) |
0 (0.0%) |
1 (2.1%) |
0 (0.0%) |
|
Endocrine |
|
|
|
|
|
|
|
|
|
|
|
Hypothyroidism |
61 (14.6%) |
2 (2.1%) |
7 (18.9%) |
21 (63.6%) |
5 (8.7%) |
4 (20%) |
4 (13.3%) |
0 (0.0%) |
14 (29.1%) |
4 (7%) |
|
Hyperthyroidism |
18 (4.3%) |
7 (7.2%) |
3 (8.1%) |
0 (0.0%) |
4 (7.0%) |
0 (0.0%) |
2 (6.6%) |
0 (0.0%) |
0 (0.0%) |
2 (3.5%) |
|
Hot flushes |
3 (0.7%) |
0 (0.0%) |
0 (0.0%) |
0 (0.0%) |
0 (0.0%) |
0 (0.0%) |
1 (3.3%) |
0 (0.0%) |
0 (0.0%) |
2 (3.5%) |
|
Hepatobiliary |
|
|
|
|
|
|
|
|
|
|
|
Elevated ALP, AST, AP |
162 (38.7%) |
57 (59.3%) |
0 (0.0%) |
18 (1.6%) |
27 (47.3%) |
4 (20%) |
12 (40%) |
1 (2.4%) |
43 (89.5%) |
0 (0.0%) |
|
Increased bilirubin |
15 (3.6%) |
3 (3.1%) |
0 (0.0%) |
0 (0.0%) |
4 (7.0%) |
0 (0.0%) |
0 (0.0%) |
0 (0.0%) |
8 (16.6%) |
0 (0.0%) |
|
Increased lipase |
28 (6.7%) |
0 (0.0%) |
0 (0.0%) |
0 (0.0%) |
17 (29.8%) |
0 (0.0%) |
3 (10%) |
8 (19.5%) |
0 (0.0%) |
0 (0.0%) |
|
Increased serum amylase |
16 (3.8%) |
0 (0.0%) |
0 (0.0%) |
0 (0.0%) |
11 (19.2%) |
3 (15%) |
2 (6.6%) |
0 (0.0%) |
0 (0.0%) |
0 (0.0%) |
|
Respiratory |
|
|
|
|
|
|
|
|
|
|
|
Cough |
65 (15.5%) |
24 (25.0%) |
3 (8.1%) |
11 (33%) |
7 (12.2%) |
3 (15%) |
1 (3.3%) |
9 (22%) |
7 (14.6%) |
0 (0.0%) |
|
Dyspnea |
57 (13.6%) |
19 (19.8%) |
4 (10.8%) |
0 (0.0%) |
10 (17.5%) |
0 (0.0%) |
4 (13.3%) |
11 (26.8%) |
9 (18.7%) |
0 (0.0%) |
|
Hemoptysis |
7 (1.7%) |
0 (0.0%) |
4 (10.8%) |
3 (9.1%) |
0 (0.0%) |
0 (0.0%) |
0 (0.0%) |
0 (0.0%) |
0 (0.0%) |
0 (0.0%) |
|
Nasopharyngeal congestion |
18 (4.3%) |
0 (0.0%) |
0 (0.0%) |
18 (54.5%) |
0 (0.0%) |
0 (0.0%) |
0 (0.0%) |
0 (0.0%) |
0 (0.0%) |
0 (0.0%) |
|
Pneumothorax |
3 (0.7%) |
1 (1%) |
1 (2.7%) |
1 (3.0%) |
0 (0.0%) |
0 (0.0%) |
0 (0.0%) |
0 (0.0%) |
0 (0.0%) |
0 (0.0%) |
|
Nervous system |
|
|
|
|
|
|
|
|
|
|
|
Vertigo |
1 (0.2%) |
0 (0.0%) |
0 (0.0%) |
0 (0.0%) |
0 (0.0%) |
0 (0.0%) |
1 (3.3%) |
0 (0.0%) |
0 (0.0%) |
0 (0.0%) |
|
Headache |
55 (13.1%)
|
9 (9.4%) |
4 (10.8%) |
5 (15.1%) |
7 (12.2%) |
0 (0.0%) |
2 (6.6%) |
10 (24.3%) |
18 (37.5%)
|
0 (0.0%) |
|
Cognitive disturbance |
5 (1.2%) |
4 (4.1%) |
0 (0.0%) |
0 (0.0%) |
0 (0.0%) |
0 (0.0%) |
0 (0.0%) |
0 (0.0%) |
1 (2.0%) |
0 (0.0%) |
|
Seizure |
2 (0.4%) |
0 (0.0%) |
0 (0.0%) |
2 (6.1%) |
0 (0.0%) |
0 (0.0%) |
0 (0.0%) |
0 (0.0%) |
0 (0.0%) |
0 (0.0%) |
|
Dysguisia |
22 (5.3%) |
0 (0.0%) |
10 (27%) |
0 (0.0%) |
12 (21.0%) |
0 (0.0%) |
0 (0.0%) |
0 (0.0%) |
0 (0.0%) |
0 (0.0%) |
|
Cardiac-related |
|
|
|
|
|
|
|
|
|
|
|
Chest pain |
1 (0.2%) |
0 (0.0%) |
0 (0.0%) |
0 (0.0%) |
0 (0.0%) |
0 (0.0%) |
0 (0.0%) |
0 (0.0%) |
1 (2.1%) |
0 (0.0%) |
|
Left ventricular dysfunction |
1 (0.2%) |
0 (0.0%) |
0 (0.0%) |
0 (0.0%) |
0 (0.0%) |
0 (0.0%) |
0 (0.0%) |
0 (0.0%) |
1 (2.1%) |
0 (0.0%) |
|
Pericarditis |
1 (0.2%) |
0 (0.0%) |
0 (0.0%) |
0 (0.0%) |
0 (0.0%) |
0 (0.0%) |
0 (0.0%) |
0 (0.0%) |
1 (2.1%) |
0 (0.0%) |
|
Cardiac arrest |
1 (0.2%) |
0 (0.0%) |
0 (0.0%) |
0 (0.0%) |
1 (1.75%) |
0 (0.0%) |
0 (0.0%) |
0 (0.0%) |
0 (0.0%) |
0 (0.0%) |
| Vascular-related | ||||||||||
|
Hypertension |
46 (11.0%) |
3 (3.1%) |
0 (0.0%) |
16 (48.4%) |
0 (0.0%) |
0 (0.0%) |
0 (0.0%) |
0 (0.0%) |
27 (56%) |
0 (0.0%) |
|
Thromboembolic event |
7 (1.7%) |
4 (4.2%) |
0 (0.0%) |
0 (0.0%) |
0 (0.0%) |
0 (0.0%) |
0 (0.0%) |
0 (0.0%) |
3 (6.2%) |
0 (0.0%) |
|
Dermatological |
|
|
|
|
|
|
|
|
|
|
|
Skin rash |
15 (3.6%) |
0 (0.0%) |
6 (16.2%) |
9 (27.2%) |
0 (0.0%) |
0 (0.0%) |
0 (0.0%) |
0 (0.0%) |
0 (0.0%) |
0 (0.0%) |
|
Maculopapular rash |
40 (9.5%) |
4 (4.2%) |
4 (2.7%) |
0 (0.0%) |
12 (21.0%) |
0 (0.0%) |
9 (30%) |
0 (0.0%) |
11 (23%) |
0 (0.0%) |
|
Dry skin |
2 (0.4%) |
0 (0.0%) |
0 (0.0%) |
0 (0.0%) |
0 (0.0%) |
0 (0.0%) |
2 (6.6%) |
0 (0.0%) |
0 (0.0%) |
0 (0.0%) |
|
Pruritus |
37 (8.8%) |
6 (6.2%) |
9 (24.3%) |
9 (27.2%) |
6 (10.5%) |
4 (20%) |
1 (3.3%) |
0 (0.0%) |
0 (0.0%) |
2 (3.5%) |
|
Alopecia |
28 (6.7%) |
0 (0.0%) |
14 (42.4%) |
0 (0.0%) |
14 (24.5%) |
0 (0.0%) |
0 (0.0%) |
0 (0.0%) |
0 (0.0%) |
0 (0.0%) |
|
Palmar-Plantar-erythrodysthesia syndrome |
10 (2.4%) |
0 (0.0%) |
0 (0.0%) |
0 (0.0%) |
0 (0.0%) |
0 (0.0%) |
0 (0.0%) |
0 (0.0%) |
10 (21%) |
0 (0.0%) |
|
Metabolic and nutritional |
|
|
|
|
|
|
|
|
|
|
|
Hypoalbuminemia |
36 (8.6%) |
21 (21.8%) |
0 (0.0%) |
0 (0.0%) |
9 (0.0%) |
0 (0.0%) |
0 (0.0%) |
6 (14.6%) |
0 (0.0%) |
0 (0.0%) |
|
Hypokalemia |
24 (5.7%) |
11 (11.4%) |
0 (0.0%) |
0 (0.0%) |
7 (0.0%) |
0 (0.0%) |
0 (0.0%) |
6 (14.6%) |
0 (0.0%) |
0 (0.0%) |
|
Hypomagnesmia |
22 (5.2%) |
0 (0.0%) |
6 (16.2%) |
0 (0.0%) |
13 (0.0%) |
0 (0.0%) |
3 (10%) |
0 (0.0%) |
0 (0.0%) |
0 (0.0%) |
|
Hypophosphatemia |
24 (5.7%) |
3 (3.1%) |
0 (0.0%) |
0 (0.0%) |
11 (0.0%) |
0 (0.0%) |
2 (6.6%) |
8 (19.5%) |
0 (0.0%) |
0 (0.0%) |
|
Hypertriglyceridemia |
3 (0.7%) |
0 (0.0%) |
0 (0.0%) |
3 (9.1%) |
0 (0.0%) |
0 (0.0%) |
0 (0.0%) |
0 (0.0%) |
0 (0.0%) |
0 (0.0%) |
|
Investigations |
|
|
|
|
|
|
|
|
|
|
|
Decreased WBC count |
48 (11.4%)
|
0 (0.0%) |
3 (8.1%) |
0 (0.0%) |
31(54.3%) |
0 (0.0%) |
0 (0.0%) |
0 (0.0%) |
14 (29.1%) |
0 (0.0%) |
|
Decreased neutrophil count |
47 (11.2%) |
0 (0.0%) |
9 (24%) |
0 (0.0%) |
32(56.1%) |
0 (0.0%) |
0 (0.0%) |
6 (14.6%) |
0 (0.0%) |
0 (0.0%) |
|
Elevated hemoglobin |
5 (1.2%) |
0 (0.0%) |
0 (0.0%) |
5 (15.0%) |
0(0.0%) |
0 (0.0%) |
0 (0.0%) |
0 (0.0%) |
0 (0.0%) |
0 (0.0%) |
|
Increased creatinine or BUN |
10 (2.4%) |
0 (0.0%) |
0 (0.0%) |
6 (18.1%) |
4(7.0%) |
0 (0.0%) |
0 (0.0%) |
0 (0.0%) |
0 (0.0%) |
0 (0.0%) |
|
Decreased ejection fraction |
2 (0.4%) |
0 (0.0%) |
2 (5.4%) |
0 (0.0%) |
0(0.0%) |
0 (0.0%) |
0 (0.0%) |
0 (0.0%) |
0 (0.0%) |
0 (0.0%) |
|
MSK-Connective tissue-related |
|
|
|
|
|
|
|
|
|
|
|
Myalgia |
25 (6.0%) |
6 (6.2%) |
0 (0.0%) |
0 (0.0%) |
7 (12.2%) |
0 (0.0%) |
4 (13.3%) |
5 (12.1%) |
0 (0.0%) |
3 (5.2%) |
|
Arthralgia |
49 (11.6%) |
7 (7.3%) |
0 (0.0%) |
15 (45.4%) |
9 (15.7%) |
0 (0.0%) |
6 (20%) |
7 (17.1%) |
0 (0.0%) |
5 (8.7%) |
|
General |
|
|
|
|
|
|
|
|
|
|
|
Fatigue |
217 (51.8%) |
34 (35.4%) |
21 (56.7%) |
26 (78.7%) |
41 (72.0%) |
16 (80%) |
10 (33.3%) |
15 (36.5%) |
25 (52%) |
29(50.8%) |
|
Weight loss |
55 (13.1%) |
18 (18.7%) |
6 (16.2%) |
12 (36.3%) |
17 (29.8%) |
0 (0.0%) |
2 (6.6%) |
0 (0.0%) |
0 (0.0%) |
0 (0.0%) |
|
Fever |
34 (8.1%) |
0 (0.0%) |
7 (19%) |
0 (0.0%) |
14 (24.5%) |
0 (0.0%) |
9 (30%) |
2 (4.8%) |
0 (0.0%) |
2 (3.5%) |
|
Insomnia |
13 (3.1%) |
7 (7.3%) |
0 (0.0%) |
0 (0.0%) |
3 (5.2%) |
1 (5%) |
2 (6.6%) |
0 (0.0%) |
0 (0.0%) |
0 (0.0%) |
|
Tumor pain |
52 (12.4%) |
1 (1.0%) |
0 (0.0%) |
15 (45.4%) |
6 (10.5%) |
0 (0.0%) |
0 (0.0%) |
0 (0.0%) |
0 (0.0%) |
30(52.6%) |
|
Ocular |
|
|
|
|
|
|
|
|
|
|
|
Dry eye |
8 (2.0%) |
0 (0.0%) |
8 (21.6%) |
0 (0.0%) |
0 (0.0%) |
0 (0.0%) |
0 (0.0%) |
0 (0.0%) |
0 (0.0%) |
0(0.0%) |
|
Optic neuritis/uveitis |
1 (0.2%) |
0 (0.0%) |
0 (0.0%) |
0 (0.0%) |
0 (0.0%) |
0 (0.0%) |
1 (3.3%) |
0 (0.0%) |
0 (0.0%) |
0(0.0%) |
|
Infection |
|
|
|
|
|
|
|
|
|
|
|
Oral mucositis |
52 (12.4%) |
0 (0.0%) |
13 (35.1%) |
23 (69.6%) |
11 (19.2%) |
0 (0.0%) |
1 (3.3%) |
0 (0.0%) |
0 (0.0%) |
4(7.0%) |
|
Pericarditis |
1 (0.2%) |
0 (0.0%) |
0 (0.0%) |
0 (0.0%) |
0 (0.0%) |
0 (0.0%) |
0 (0.0%) |
0 (0.0%) |
1 (2.1%) |
0(0.0%) |
|
Rectal or vaginal mucositis |
7 (1.7%) |
0 (0.0%) |
1 (2.7 %) |
6 (18.1%) |
0 (0.0%) |
0 (0.0%) |
0 (0.0%) |
0 (0.0%) |
0 (0.0%) |
0(0.0%) |
|
URTI |
4 (1.0%) |
0 (0.0%) |
4 (10.8%) |
0 (0.0%) |
0 (0.0%) |
0 (0.0%) |
0 (0.0%) |
0 (0.0%) |
0 (0.0%) |
0(0.0%) |
|
Immune-related |
|
|
|
|
|
|
|
|
|
|
|
Hyperglycemia |
34 (8.1%) |
17 (17.7%) |
0 (0.0%) |
9 (27.2%)
|
8 (14.0%) |
0 (0.0%) |
0 (0.0%) |
0 (0.0%) |
0 (0.0%) |
0(0.0%) |
|
Autoimmune colitis |
1 (0.2%) |
0 (0.0%) |
0 (0.0%) |
1 (3.0%) |
0 (0.0%) |
0 (0.0%) |
0 (0.0%) |
0 (0.0%) |
0 (0.0%) |
0(0.0%) |
|
Autoimmune hepatitis |
2 (0.4%) |
0 (0.0%) |
0 (0.0%) |
1 (3.0%) |
0 (0.0%) |
0 (0.0%) |
0 (0.0%) |
1 (2.4%) |
0 (0.0%) |
0(0.0%) |
|
Autoimmune arthritis |
3 (0.7%) |
0 (0.0%) |
0 (0.0%) |
2 (6.0%) |
0 (0.0%) |
0 (0.0%) |
1 (3.3%) |
0 (0.0%) |
0 (0.0%) |
0(0.0%) |
|
Pulmonary embolism |
1 (0.2%) |
1 (1.0%) |
0 (0.0%) |
0 (0.0%) |
0 (0.0%) |
0 (0.0%) |
0 (0.0%) |
0 (0.0%) |
0 (0.0%) |
0(0.0%) |
|
Adrenal insufficiency |
1 (0.2%) |
1 (1.0%) |
0 (0.0%) |
0 (0.0%) |
0 (0.0%) |
0 (0.0%) |
0 (0.0%) |
0 (0.0%) |
0 (0.0%) |
0(0.0%) |
|
Pneumonitis |
10 (2.4%) |
2 (2.1%) |
0 (0.0%) |
0 (0.0%) |
2 (3.5%) |
4 (20%) |
2 (6.6%) |
0 (0.0%) |
0 (0.0%) |
0(0.0%) |
|
Interstitial nephritis |
1 (0.2%) |
1 (1.0%) |
0 (0.0%) |
0 (0.0%) |
0 (0.0%) |
0 (0.0%) |
0 (0.0%) |
0 (0.0%) |
0 (0.0%) |
0(0.0%) |
| * The percentages were calculated by dividing by the total number of enrolled patients (419), **The numbers between the parentheses represent the number of enrolled patients, URTI: Upper respiratory tract infection, Pemb: Pembrolizumab. | ||||||||||
Compared to pembrolizumab monotherapy, combination therapy was associated with significantly better tumor responses, including higher rates of partial and stable disease and a lower incidence of progressive disease (p < 0.001). Hematological toxicities differed significantly: thrombocytopenia was more frequent with combination therapy (p = 0.010), while lymphopenia and anemia were more common with monotherapy (p < 0.001 and p = 0.001, respectively). Gastrointestinal events such as nausea (p = 0.019), xerostomia (p = 0.001), and abdominal pain (p = 0.003) were also more common in combination therapy. Combination therapy was linked to higher rates of hypothyroidism (p < 0.001), hepatobiliary abnormalities, including elevated liver enzymes (p < 0.001), lipase (p = 0.001), and amylase (p = 0.029). Respiratory (cough: p = 0.006; rhinorrhea: p = 0.018), neurological (dysgeusia: p = 0.004), vascular (hypertension: p = 0.005), and dermatological toxicities (skin rash: p = 0.028; maculopapular rash: p = 0.047; alopecia: p = 0.001) were also significantly higher in combination therapy. Metabolic disturbances such as hypoalbuminemia (p < 0.001), hypokalemia (p = 0.011), and hypomagnesemia (p = 0.004) varied between groups. Additionally, adverse events such as decreased WBC and neutrophil counts, fatigue, tumor pain, and oral mucositis were more common in the combination group (p < 0.001), whereas insomnia (p = 0.014) and hyperglycemia (p < 0.001) were more frequent with monotherapy (Table 6).
|
Parameters |
Type of therapy |
P-value |
|
|
Pembrolizumab Alone |
Combination Therapy |
||
|
Progression-free survival, Days (Median, IQR) |
56.0 (75.0) |
103.5 (112.0) |
0.303 |
|
Overall survival, Days (Median, IQR) |
343 (201.0) |
417 (263.5) |
0.559 |
|
Outcome (N, %) * Complete response Partial response Stable disease Progressive disease |
1 (1.1) 8 (8.7) 24 (26.1) 59 (64.1) |
1 (0.4) 48 (17.6) 120 (44.1) 103 (37.9) |
<0.001 |
|
Hematological adverse events Thrombocytopenia Lymphopenia Febrile Neutropenia Anemia |
0 (0.0) 26 (27.1) 4 (4.2) 43 (44.8) |
19 (5.9) 10 (3.1) 9 (2.8) 83 (25.7) |
0.010 <0.001 0.506 0.001 |
|
Gastrointestinal adverse events Nausea Vomiting Anorexia Constipation Diarrhea Decreased Appetite Xerostomia Abdominal Pain Colitis |
22 (22.9) 11 (11.5) 14 (14.6) 17 (17.7) 15 (15.6) 0 (0.0) 0 (0.0) 13 (13.5) 0 (0.0) |
116 (35.9) 45 (13.9) 58 (18.0) 38 (11.8) 81 (25.1) 7 (2.2) 26 (8.0) 14 (4.3) 5 (1.5) |
0.019 0.611 0.538 0.167 0.054 0.359 0.001 0.003 0.593 |
|
Endocrine adverse events Hypothyroidism Hyperthyroidism |
2 (2.1) 7 (7.3) |
59 (18.3) 11 (3.4) |
<0.001 0.146 |
|
Hepatobiliary adverse events Elevated ALP, AST, ALT Elevated Bilirubin Elevated Lipase Elevated Serum Amylase |
3 (3.1) 0 (0.0) 0 (0.0) |
105 (32.5) 12 (3.7) 28 (8.7) 16 (5.0) |
<0.001 0.999 0.001 0.029 |
|
Respiratory adverse events Cough Dyspnea Hemoptysis Rhinorrhea Pneumothorax |
19 (19.8) 0 (0.0) 0 (0.0) 1 (1.0) |
41 (12.7) 38 (11.8) 7 (2.2) 18 (5.6) 2 (0.6) |
0.006 0.061 0.359 0.018 0.543 |
|
Neurological adverse events Headache Dysgeusia |
0 (0.0) |
46 (14.2) 22 (6.8) |
0.301 0.004 |
|
Vascular adverse events Hypertension |
|
43 (13.3) |
0.005 |
|
Dermatological adverse events Skin Rash Maculopapular Rash Dry Skin Pruritus Alopecia |
0 (0.0) 4 (4.2) 0 (0.0) 6 (6.3) 0 (0.0) |
15 (4.6) 36 (11.1) 2 (0.6) 31 (9.6) 28 (8.7) |
0.028 0.047 0.999 0.413 0.001 |
|
Metabolic and nutritional adverse events Hypoalbuminemia Hypokalemia Hypomagnesemia Hypophosphatemia |
21 (21.9) 11 (11.5) 0 (0.0) 3 (3.1) |
15 (4.6) 13 (4.0) 22 (6.8) 21 (6.5) |
<0.001 0.011 0.004 0.316 |
|
Musculoskeletal and connective tissue adverse events Myalgia Arthralgia |
6 (6.3) 7 (7.3) |
19 (5.9) 42 (13.0) |
0.811 0.149 |
|
Others Decreased WBC count Elevated HBG Decreased Neutrophil count Elevated Creatinine or BUN Fatigue Weight Loss Fever Insomnia Tumor pain Oral mucositis Rectal or Vaginal mucositis Hyperglycemia Pneumonitis |
0 (0.0) 0 (0.0) 0 (0.0) 0 (0.0) 34 (35.4) 18 (18.8) 0 (0.0) 7 (7.3) 1 (1.0) 0 (0.0) 0 (0.0) 17 (17.7) 1 (1.0) |
48 (14.9) 5 (1.5) 47 (14.6) 10 (3.1) 183 (56.7) 37 (11.5) 34 (10.6) 6 (1.9) 51 (15.8) 52 (16.1) 6 (1.9) 17 (5.3) 8 (2.5) |
<0.001 0.593 <0.001 0.126 <0.001 0.084 <0.001 0.014 <0.001 <0.001 0.344 <0.001 0.69 |
|
* Analyses were done for evaluable cases, IQR: Interquartile range, ALP: Alkaline phosphatase, AST: Aspartate aminotransferase, ALT: Alanine Aminotransferase, WBC: White blood cells, HBG: Hemoglobin, BUN: Blood Urea Nitrogen |
|||
Discussion
The current meta-analysis results demonstrate a stark contrast between pembrolizumab monotherapy and combination approaches in sarcoma treatment. With pembrolizumab monotherapy showing an 83% progressive disease rate compared to 36% with combination therapy, these findings suggest that immune checkpoint inhibitors alone might have limited efficacy in most sarcoma subtypes. However, there is considerable heterogeneity between the studies (I² = 93.3% for monotherapy and I² = 82.7% for combination therapy), reflecting significant differences in histologic subtypes, patient selection, treatment regimens, and tumor biology. The wide prediction interval (0.00–1.00) indicates uncertainty regarding the reproducibility of these results in future studies. Although this introduces variability, it reflects inherent differences across study populations or methodologies rather than undermining the overall consistency and reliability of the core findings.
The SARC028 trial, evaluating pembrolizumab monotherapy in sarcomas, reported an ORR of 18% in soft tissue sarcomas, with responses primarily observed in undifferentiated pleomorphic sarcoma and liposarcoma [9]. This contrasts with Boye et al’s finding of 0% ORR in a cohort of 12 patients treated with pembrolizumab alone, highlighting the variability in treatment responses across different sarcoma subtypes and patient populations [7]. The limited efficacy of pembrolizumab monotherapy is further supported by the AcSé trial, which reported an ORR of only 6.2% across various rare sarcoma subtypes [18].
The significant variability in treatment outcomes across different histological subtypes underscores the importance of histology-specific approaches in sarcoma management. The current analysis revealed that leiomyosarcoma was the most common histological subtype, yet previous studies have shown this subtype to be relatively resistant to immune checkpoint inhibition. The SARC028 trial reported no responses in leiomyosarcoma patients treated with pembrolizumab monotherapy. In contrast, certain histological subtypes have demonstrated greater sensitivity to immunotherapy. For instance, undifferentiated pleomorphic sarcoma has shown a 40% ORR [9]. Similarly, alveolar soft part sarcoma has emerged as a particularly responsive subtype, with studies reporting response rates of up to 50% with PD-1 inhibition. These findings highlight the critical importance of histology-specific patient selection for immunotherapy trials in sarcoma [19].
The current meta-analysis demonstrated that combination approaches significantly improve treatment outcomes compared to pembrolizumab monotherapy, with combination therapy showing a 64% lower rate of progressive disease. This substantial improvement suggests that combining immune checkpoint inhibitors with other therapeutic modalities may overcome some of the inherent resistance mechanisms in sarcomas.
The combination of pembrolizumab with doxorubicin showed an ORR of 19% [10]. This combination demonstrated manageable toxicity and promising activity. The synergistic effect may be attributed to chemotherapy-induced immunogenic cell death, which can enhance T-cell priming and activation, potentially converting "cold" tumors into "hot" immunogenic ones [20]. The combinations of pembrolizumab with axitinib and lenvatinib showed ORRs of 25% and 15.2%, respectively [11,12]. Wilky et al. reported that axitinib plus pembrolizumab demonstrated manageable toxicity and preliminary activity in advanced sarcomas, particularly in alveolar soft part sarcoma, with a 3-month progression-free survival rate of 65.6% [11]. Similarly, a trial of lenvatinib plus pembrolizumab showed promising activity in certain sarcoma subtypes, including undifferentiated pleomorphic sarcoma and liposarcoma, and malignant peripheral nerve sheath tumors [12]. The enhanced efficacy of these combinations may be attributed to the immunomodulatory effects of tyrosine kinase inhibitors, particularly those targeting VEGF pathways [11].
Novel combination approaches, such as pembrolizumab with talimogene laherparepvec, showed the highest ORR at 35%. Talimogene laherparepvec is an oncolytic virus that can induce immunogenic cell death and enhance systemic anti-tumor immunity, potentially synergizing with immune checkpoint inhibition [13]. In contrast, the combination of pembrolizumab with epacadostat showed an ORR of 3.3%. Epacadostat is an Indoleamine 2,3-dioxygenase 1 inhibitor that was initially thought to complement immune checkpoint inhibition by targeting a different immunosuppressive pathway. However, this combination has shown limited efficacy across multiple tumor types, suggesting that IDO1 inhibition may not be a viable strategy for enhancing immunotherapy responses in sarcomas [14].
The current analysis revealed significant differences in the toxicity profiles between pembrolizumab monotherapy and combination therapy. While combination therapy was associated with better tumor responses, it also resulted in a higher incidence of certain adverse events, particularly thrombocytopenia, hypothyroidism, and hepatobiliary abnormalities. This is consistent with previous studies showing that combining immune checkpoint inhibitors with other therapeutic agents often increases toxicity. A meta-analysis of 18 studies with 2,767 patients found that the risk of severe (grade 3 or higher) adverse events was more than double for combination therapy (risk ratio 2.21, 95% CI 1.57–3.10) [21].
The significant heterogeneity in treatment responses observed in the current analysis and previous studies underscores the need for a personalized approach to sarcoma management. For example, the recent UK guidelines for soft tissue sarcoma management emphasize that certain sarcoma subtypes, such as Ewing sarcoma and rhabdomyosarcoma, require distinct treatment approaches [22].
While the current analysis showed improved outcomes with combination therapy compared to pembrolizumab monotherapy, there is still significant room for improvement. Novel combination strategies targeting multiple aspects of tumor biology and the immune microenvironment may further enhance treatment outcomes [19]. Combinations of immune checkpoint inhibitors with radiation therapy have shown promise in preclinical studies and early clinical trials. Radiation can induce immunogenic cell death, increase neoantigen presentation, and enhance T-cell infiltration, potentially synergizing with immune checkpoint inhibition [19]. Despite initial responses, many patients eventually develop resistance to immunotherapy. Understanding the mechanisms of primary and acquired resistance is crucial for developing effective strategies to overcome resistance. Potential mechanisms include loss of tumor antigens, upregulation of alternative immune checkpoints, and recruitment of immunosuppressive cells to the tumor microenvironment [23].
Conclusion
Pembrolizumab-based combination therapies have the potential to enhance treatment efficacy in sarcoma, although they may be associated with an increased risk of adverse events.
Declarations
Conflicts of interest: The authors have no conflicts of interest to disclose.
Ethical approval: Not applicable.
Consent for participation: Not applicable.
Consent for publication: Not applicable.
Funding: The present study received no financial support.
Acknowledgements: None to be declared.
Authors' contributions: RMA, SSO, SHA, SRH and MMA: major contributors to the conception of the study, as well as the literature search for related studies, and manuscript writing. FHF, HMH, AMM, SOQ, YMM and ADA: Literature review, design of the study, critical revision of the manuscript, and processing of the tables. AGH, DOQ, and MMA: Literature review, processing of the figures, data analysis and interpretation. All authors have read and approved the final version of the manuscript.
Use of AI: ChatGPT-3.5 was used to assist with language refinement and improve the overall clarity of the manuscript. All content was thoroughly reviewed and approved by the authors, who bear full responsibility for the final version.
Data availability statement: Not applicable.
Review Articles
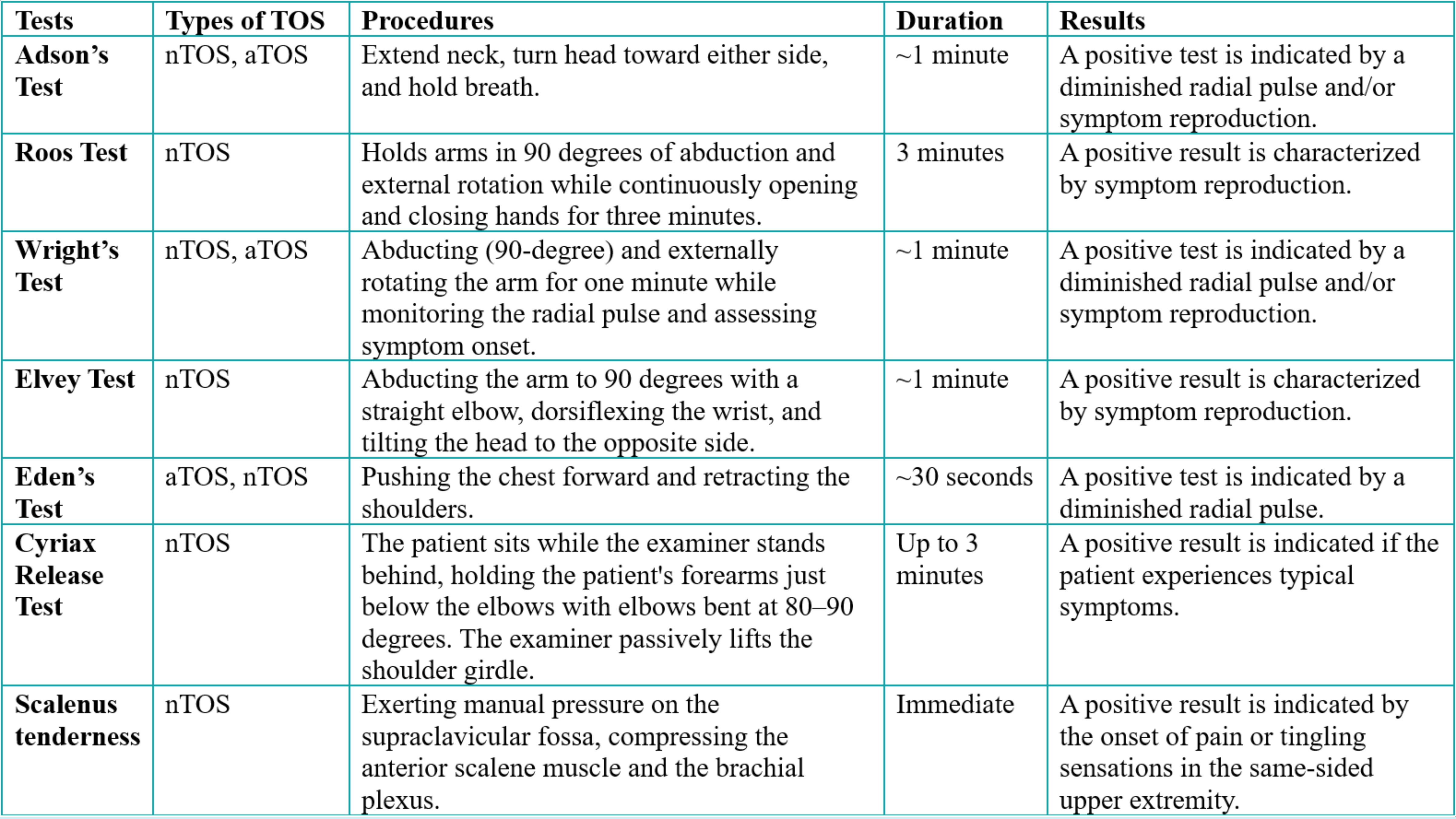
Case Reports
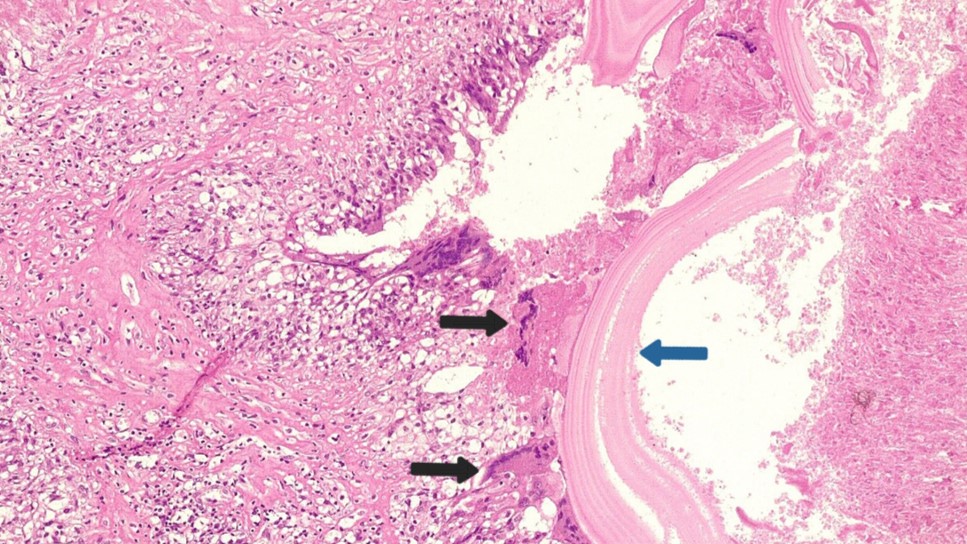
Pediatric Adrenal Hydatid Cyst: A Case Report and Literature Review
Wirya N. Sabir, Hadeel A. Yasseen, Shwan F. Abdulaziz, Paiwand A. Nadr, Shaho F. Ahmed, Meer M....
Abstract
Introduction: Echinococcosis is a zoonotic disease that can affect various organs and tissues in the human body. However, primary adrenal hydatid cyst (AHC) is rare and may be overlooked, making its early detection crucial. This report presents a case of an incidentally diagnosed primary AHC.
Methods: A 5-year-old female with an unremarkable medical history underwent abdominal ultrasonography for assessment of an inguinal hernia, and a right adrenal lesion was incidentally discovered. Intraoperatively, the lesion was suspected to be AHC, which was later confirmed by histopathology.
Results: The 10 cases of AHC that were reviewed had a mean age of 46.2 ± 12.2 years; six patients were male. Three cases had a history of contact with animals. No laterality differences were observed, and the mean cyst size was 7.45 ± 2.7 cm. Flank pain was the most common symptom (3 of 10), and surgery was performed for all the cases, accompanied by antiparasitic drugs in five cases. No cases of recurrence were reported.
Conclusion: Primary AHC can be easily overlooked or misdiagnosed as an adrenal mass, often being identified incidentally during investigations for unrelated health concerns. Surgical excision of the cyst without rupture may yield favorable results.
Introduction
Echinococcosis is a widely recognized zoonotic disease caused by the larval form of the tapeworm Echinococcus granulosus [1]. Although the disease can occur globally, it is considered endemic in several regions, including the Middle East, the Mediterranean basin, parts of South America, South Africa, and Australia [1]. Humans serve as accidental intermediate hosts for the parasite, acquiring the infection through direct contact with definitive hosts (such as dogs) or via ingestion of food or water contaminated with feces that contain parasitic eggs, often originating from livestock environments involving sheep, goats, or cattle [2]. Major risk factors include close contact with dogs, involvement in livestock activities, and living in endemic areas [2]. The prevalence of hydatid cysts in children differs by region, with a reported incidence of 2-6 cases per 100,000 children affecting individuals as young as six months old. Human infections typically occur incidentally through the ingestion of parasite eggs in contaminated food or water or by direct contact with infected hosts [3,4]. Hydatid cysts (HCs) are typically found in the liver and lungs, while the adrenal gland is a rare and unusual site of involvement [5]. This report presents a case of a primary adrenal HC (AHC) that was incidentally diagnosed in a child. The references cited in this report have been reviewed to ensure the exclusion of any non-peer-reviewed data, and the study has been structured following the CaReL guidelines [6,7].
Case presentation
Patient information and clinical findings
A 5-year-old girl presented with a two-month history of reducible inguinal swelling on the left side. She had undergone a left inguinal herniotomy nine months earlier. The swelling, consistent with a recurrent inguinal hernia, increased in size during episodes of coughing or crying. Otherwise, her past medical history was unremarkable. She belonged to a socioeconomically poor family with limited education and resided in an urban area. Notably, her grandfather, who lived in a rural area and had direct contact with animals, had a history of HC.
Diagnostic approach
Ultrasonography was performed to rule out a right-sided inguinal hernia. Incidentally, it revealed a well-defined 30 × 20 mm lesion with a central cystic area between the right kidney's upper pole and the liver's right lobe, suggesting an adrenal lesion. Five days later, a follow-up ultrasound conducted by another radiologist identified a similar well-defined lesion measuring 31 × 19 mm. Subsequently, the patient was referred to a pediatric hematologist for further evaluation. Laboratory investigations revealed a normal complete blood count. Urinalysis indicated the presence of mucus, while aspartate aminotransferase (38 IU/L, Normal range: 15–40 IU/L) was borderline elevated, lactate dehydrogenase (370 IU/L, Normal range: 100–250 IU/L ), and erythrocyte sedimentation rate (28 mm/hr, Normal range: 0–10 mm/hr) were elevated. Computed tomography (CT) of the chest and abdomen demonstrated a well-defined, irregular, heterogeneous mass in contact with the right adrenal gland, with evidence of invasion into segment VII of the liver and involvement of the posterior right hemidiaphragm (Figure 1).
Therapeutic intervention
Following a multidisciplinary discussion, the patient underwent surgery under general anesthesia. The procedure involved complete resection of the mass through a 10cm right subcostal incision, along with the excision of several ipsilateral lymph nodes for histopathological analysis (Figure 2). Subsequently, a left-sided herniotomy for the recurrent hernia was performed. Albendazole was administered postoperatively.
Follow-up
On the eighth postoperative day, the surgical wound was clean and dry. Histopathological examination revealed an infected wall of HC, accompanied by a granulomatous reaction, with adherent and compressed adrenal and liver tissue (Figure 3). Additionally, the ipsilateral lymph nodes exhibited reactive follicular hyperplasia. The patient's recovery was uneventful, and she remains under ongoing follow-up care.
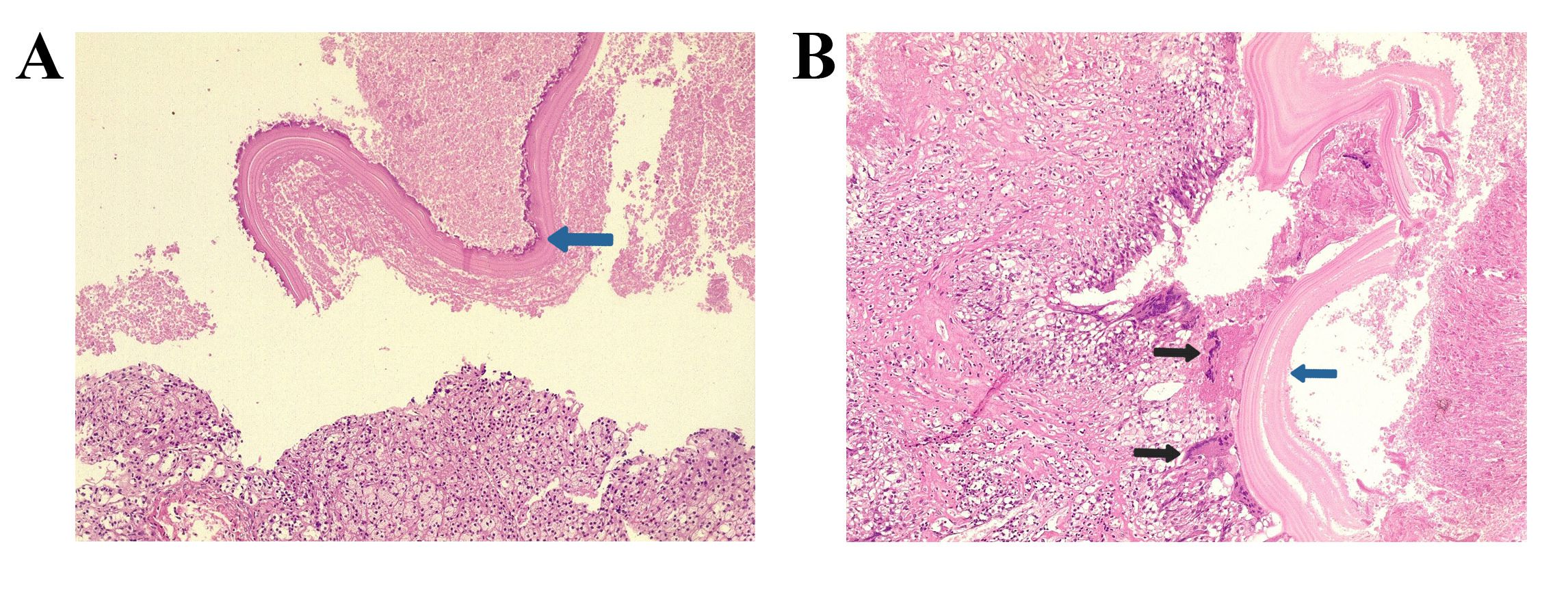
Discussion
Four distinct types of Echinococcus have been recognized as responsible for hydatid disease in humans, with E. granulosus being the most commonly encountered type (95%) [8]. The disease can affect all organs and tissues in the human body [9]. The mechanism behind adrenal involvement remains unclear. The most plausible theory suggests that once the larvae exit the digestive system, they pass through the hepatic filter to reach the lungs. If they evade destruction by the immune system or are not trapped in the filtration system, they can spread out to the unusual sites of the body, such as the spleen, kidneys, brain, bones, heart, muscle tissue, pancreas, retroperitoneum, thyroid, and adrenal glands via the arterial circulation [5]. Larvae can also disseminate through systemic circulation via lymphatic vessels or direct adjacent contact [5]. AHC is a rare entity, accounting for only 0.073% of all hydatid cyst cases [9].
While individuals of all ages can be affected, this condition is more frequently seen in those aged 50 to 60, with a slightly higher prevalence in women [10]. However, the 10 reviewed cases had a mean age of 46.2 ± 12.2 years; six patients were male. The youngest case was an 18-year-old male, and the oldest was a 64-year-old male [5, 8-16]. The present case was only a 5-year-old female, which seems to be an infrequent age for this disease. Children can contract the infection through several pathways, such as direct contact with infected animals or consuming contaminated food or water. Furthermore, the higher prevalence of HCs in endemic areas accounts for the increased incidence in younger age groups.
The disease typically presents as unilateral in 92% of cases and does not exhibit a preference for either side [11]. This is supported by the fact that the disease was unilateral in all 10 cases reviewed in this report, with no differences in laterality observed (Table 1) [5, 8-16]. HCs are typically asymptomatic and often found incidentally during imaging studies for other reasons. They seldom lead to complications and usually become symptomatic primarily due to pressure-related effects [8].
|
Author /year [reference] |
Age (Y) |
Sex |
Country |
Contact with animals |
Tumor size (cm) |
Side |
Symptoms |
Medical history |
Therapeutic approach |
Recurrence |
Follow-up (M) |
|
Zouari et al./ 2020 [5] |
55 |
N/A |
Tunisia |
N/A |
12 |
Left |
Left hypochondrium pain |
None |
Surgery |
N/A |
N/A |
|
Tajmalzai et al./ 2025 [8] |
18 |
M |
Afghanistan |
Yes |
5.2 |
Right |
Right side flank pain |
None |
Albendazole & Surgery |
No |
N/A |
|
Agarwal et al./2024 [9] |
38 |
M |
India |
N/A |
6.8 |
Right |
Vague abdominal pain |
None |
Surgery & Albendazole |
No |
12 |
|
Staouni et al./ 2022 [10] |
46 |
F |
Morocco |
N/A |
6 |
Left |
Left hypochondrial pain |
None |
Surgery |
No |
12 |
|
Salih et al./ 2018 [11] |
48 |
F |
United Arab Emirates |
Yes |
7.2 |
Left |
Large palpable mass, moderate left loin pain |
None |
Laparoscopic surgery |
N/A |
N/A |
|
Tazi et al./ 2012 [12] |
64 |
M |
Morocco |
No
|
11.3 |
Left |
Left flank pain nausea & vomiting |
Arterial hypertension |
Surgery |
No |
24 |
|
Elzein et al./ 2016 [13] |
44 |
M |
Saudi Arabia |
Yes |
7.1 |
Right |
Flank pain |
N/A |
Surgery & Albendazole |
N/A |
N/A |
|
Abdulmajed et al./ 2010[14] |
48 |
F |
Turkey |
No |
5.2 |
Right |
Vague right loin pain |
Systolic hypertension |
Surgery & Albendazole |
N/A |
N/A |
|
Bouchaala et al./ 2021[15] |
46 |
M |
Tunisia |
No |
9.7 |
Right |
Non-specific abdominal pain |
Abdominal pain & weight loss |
Surgery & Albendazole |
No |
N/A |
|
Nardi et al./ 2015 [16] |
55 |
M |
Argentina |
N/A |
4 |
Left |
Back pain |
None |
Laparoscopic surgery |
N/A |
N/A |
|
M: male, F: female, N/A: non-applicable,Y: Years, M: months |
|||||||||||
The most common symptoms are pain (hypochondriac or flank pain), nausea and vomiting, and palpable mass, usually due to inflammation of adjacent tissues caused by the cyst. Systemic symptoms may also occur, such as hypertension resulting from renal artery occlusion or symptoms that mimic pheochromocytoma due to compression of the adrenal medulla by cysts [9]. The most severe complication of HCs is cyst rupture, leading to anaphylaxis and bleeding [5,10]. Flank pain was the most common presenting symptom among the reviewed cases (3 of 10), with no systemic or severe complications reported [5,8-16]. Consistent with the literature, the present case was asymptomatic, and the HC was incidentally detected as an adrenal lesion on ultrasonography performed for an inguinal hernia.
The imaging characteristics of hydatid disease vary depending on the stage of progression. Early lesions present as purely cystic, and as the germinal layer undergoes changes and intraluminal pressure decreases, the capsule becomes fibrotic and may occasionally calcify. Meanwhile, daughter cysts can detach from the wall and float within the lumen [12]. Based on the histopathological findings, which revealed a lamellated wall with cellular debris, accompanied by chronic inflammation and a foreign body giant cell reaction, the features may suggest that the cyst was in a relatively advanced or degenerative stage.
The differential diagnosis of an adrenal cyst includes an endothelial cyst, a pseudocyst caused by infarction or hemorrhage in the adrenal gland, cystic neoplasm, cystic lymphangioma, calcified hemorrhagic cyst, extra-adrenal cystic masses, and post-traumatic cysts [9]. The identification of HCs in the adrenal gland primarily relies on ultrasonography and CT scans. Ultrasound has a sensitivity of 93% to 98% for diagnosis, while CT scans achieve around 97% sensitivity [10]. Ultrasound is typically the initial examination. However, the depth of the adrenal glands and occasional peripheral calcifications can make this assessment challenging. A CT scan provides a clearer view of the location and its relationship with nearby organs [5]. Hydatid serology (such as hemagglutination and ELISA) can offer diagnostic confirmation when results are positive. However, false negative results are possible [13]. Recognizing rare presentations like adrenal involvement is clinically important to avoid misdiagnosis and utilize an appropriate therapeutic approach.
The treatment for the AHCs is primarily surgery. The two preferred options are pericystectomy and complete adrenal gland resection. However, the cyst resection while preserving the gland is considered the optimal approach [14,15]. Some authors reported that the laparoscopic approach represents a viable option due to its association with low morbidity and complication rates when performed by experienced surgeons [16]. In the present case, a CT scan was conducted following the incidental finding on ultrasonography. The scan revealed a well-defined, irregular, heterogeneous mass in contact with the right adrenal gland, with evidence of invasion into segment VII of the liver. Subsequently, the patient underwent surgery, during which the mass was completely resected. Histopathological examination confirmed the diagnosis of AHC.
Conclusion
Primary AHC can be easily overlooked or misdiagnosed as an adrenal mass, often being identified incidentally during investigations for unrelated health concerns. Surgical excision of the cyst without rupture may yield favorable results.
Declarations
Conflicts of interest: The authors have no conflicts of interest to disclose.
Ethical approval: Not applicable.
Consent for participation: Not applicable.
Consent for publication: Written informed consent for publication was obtained from the parents.
Funding: The present study received no financial support.
Acknowledgments: None to be declared.
Authors' contributions: WNS, HAY, SFA, FHK, and MMA: Major contributors to the conception of the study, as well as the literature search for related studies, and manuscript writing. SFA, HOA, BAA, and KAN: Literature review, critical revision of the manuscript, and processing of the table. PAN, SMA, and SSA: Literature review, and processing of the figures. All authors have read and approved the final version of the manuscript.
Use of AI: ChatGPT-3.5 was used to assist with language refinement and improve the overall clarity of the manuscript. All content was thoroughly reviewed and approved by the authors, who bear full responsibility for the final version.
Data availability statement: Not applicable.
Multiple Concurrent Pilonidal Sinuses: Case report and Literature review
Emad S. Siddiq, Shko H. Hassan, Abdullah A. Qadir, Meer M. Abdulkarim, Ibrahim H. Qader, Khalis...
Abstract
Introduction: Concurrent pilonidal sinuses (PNSs) at distinct locations are extremely rare. This report highlights an exceptional case of a young female presenting with three PNSs in distinct locations.
Case presentation: A 19-year-old female with a family history of PNS presented with a chronic, discharging sinus tract in the intermammary region that had persisted for two years. Physical examination revealed an erythematous lesion with intermittent purulent and bloody discharge, leading to a diagnosis of intermammary PNS (IMPNS). Surgical excision was performed, and histopathology confirmed the diagnosis. Six weeks postoperatively, the patient’s wound had completely healed; however, she mentioned symptoms in the umbilical and sacrococcyx regions that had been intermittent for the past year. Further evaluation led to diagnoses of natal cleft PNS (NCPNS) and umbilical PNS (UPNS). NCPNS was scheduled for surgical treatment, while UPNS was managed conservatively. Histopathology confirmed chronic sinus tract formation in both cases.
Literatue review: Nine cases of PNS were reviewed, six of which were males. Two of them had recurrent discharging sinuses, and no family history of PNS was reported. Locations included gluteal, auricular, mammary, cheeks, and umbilical regions. Discharge was present in all of the cases, accompanied by pain in two. Sinus excision was performed for all the cases, accompanied by laser epilation in one. Healing modalities included secondary intention and various dressings.
Conclusion: It is extremely rare for NCPNS, UPNS, and IMPNS to occur concurrently. Surgical management for NCPNS and IMPNS, combined with conservative treatment for UPNS, may lead to favorable outcomes.
Introduction
The term "pilonidal sinus" (PNS) was first introduced by Hodges in 1880. However, the condition was initially described by Anderson in 1847 as "hair extracted from an ulcer" [1]. PNS is an inflammatory disorder that occurs when hair penetrates the epidermis, leading to the formation of a blind tract lined with granulation tissue. The condition primarily affects males, with a male-to-female ratio of 4:1 [2]. It typically manifests in individuals in their late teens to early 20s and decreases in frequency after the age of 25. The risk factors for PNS are male gender, a deep natal cleft, hair in the natal cleft, a family history of the condition, jobs that require prolonged sitting, obesity, and excessive sweating. It is frequently observed in drivers, which is why it is also referred to as "Jeep disease." [2]. A large prospective case-control study found that individuals with hirsutism who sit for more than six hours a day and bathe less than twice a week have a 219-fold increased risk of developing sacrococcygeal PNS compared to those without these risk factors [3].
The incidence of PNS has significantly increased over the past 50 years for unknown reasons. It is estimated to affect 26 per 100,000 individuals [4]. PNS was initially considered a congenital condition. However, increasing reports of cases in various anatomical regions suggest it may be an acquired disorder. It most commonly develops in the sacrococcyx region, located near the base of the spine, where the skin is prone to hair accumulation and irritation. It is rarely found in the breast, intermammary region, umbilical region, endoanal area, preauricular region, neck, hand, face, penis, and clitoris [4].
The occurrence of concurrent PNSs in a single individual is an exceptionally rare condition. This report highlights a case of three concurrent PNSs located in three different cites. This report was written following the CaReL guidelines, and credible, peer reviewed sources were used, while unreliable sources were excluded [5,6].
Case presentation
Patient information
A 19-year-old female with a family history of PNS and a normal body weight presented with a chronic, discharging sinus tract in the intermammary region. The lesion had persisted for approximately two years before seeking medical consultation.
Clinical findings
On clinical examination, a small, erythematous lesion was initially observed, which had been painless at first but had progressed to form a single opening, accompanied by intermittent purulent and bloody discharge. The patient reported localized pruritus, and the surrounding skin demonstrated persistent erythema.
Diagnostic approach
The diagnosis of PNS in the intermammary region (IMPNS) was established through clinical evaluation, which included palpation of the cyst and tract, as well as assessment of drainage. Given the clear clinical presentation, no additional investigations were considered necessary.
Therapeutic intervention
The patient was scheduled for surgical excision of the sinus tract and associated abscess cavity under general anesthesia. An elliptical skin incision was made over the sinus tract to ensure complete excision while preserving surrounding healthy tissue. Sharp and blunt dissection was used to carefully remove the tract and abscess cavity down to the underlying fascia. Hemostasis was achieved using bipolar cautery. The wound was then thoroughly irrigated with povidone-iodine and normal saline. Considering the patient’s young age and cosmetic concerns, the wound was closed by primary intention using subcuticular absorbable sutures to minimize scarring and optimize the aesthetic outcome. Histopathological examination of the excised skin ellipse revealed focal surface ulceration. Within the underlying dermis, a sinus tract was identified, surrounded by a diffuse mixed inflammatory infiltrate, predominantly composed of plasma cells and neutrophils, along with granulation tissue formation. These histopathological findings, in correlation with the clinical presentation, confirmed the diagnosis of an IMPNS (Figure 1).

Follow-up
Six weeks postoperatively, the patient returned for follow-up with complete wound healing and no symptoms in the intermammary region. However, she reported new-onset pain, itching, and discharge from the umbilical and sacrococcyx areas. She disclosed a one-year history of intermittent symptoms in these regions but had previously refrained from mentioning them due to embarrassment. On examination, she was diagnosed with natal cleft PNS (NCPNS) and umbilical PNS (UPNS). The management included the Lord’s procedure for NCPNS, which involves minimal excision of the sinus openings and deroofing of the sinus tracts without removing large amounts of tissue, while UPNS was treated conservatively with hair removal and daily povidone-iodine dressing. The decision was based on the absence of secondary openings and minimal inflammation (Figure 2). Histopathology revealed focal surface ulceration and a sinus tract within the dermis, surrounded by a mixed inflammatory infiltrate predominantly composed of lymphocytes, plasma cells, foamy macrophages, and granulation tissue. These findings confirmed a chronic inflammatory lesion with sinus tract formation, characteristic of NCPNS (Figure 3).

Discussion
Typically, PNS is considered a surgical-dermatological disorder. It is a condition that contributes to the growing number of operations, particularly among young individuals. It is also part of the follicular occlusion tetrad, a group of hair follicle disorders that includes severe acne vulgaris, hidradenitis suppurativa, and dissecting cellulitis of the scalp. It affects approximately 0.07% of the general population and represents around 15% of all perianal diseases [4]. The exact cause of PNS remains uncertain, with two primary theories suggesting either an acquired or congenital origin. Generally, three factors are considered necessary for its development. The first is the presence of hair within the skin, the second is an area of wrinkled or folded skin, such as the natal cleft or a scar, and the third involves a combination of hormonal influences and hygiene-related factors [7]. The hallmark symptoms of PNS include swelling, discomfort, and discharge. Among nine cases that were reviewed, all patients exhibited discharge, while only two (22.2%) experienced pain (Table 1) [2-4,7-12]. The current patient experienced pain, itching, and discharge, which were among the common symptoms.
|
Author /year [reference] |
Age (Y) |
Sex |
Medical history |
Family history of PNS |
Location |
Symptoms |
Symptoms Duration (Y) |
Treatment |
Wound healing modality |
Outcome |
Follow-up (Y) |
|
Savant/2025 [9] |
26 |
M |
Unremarkable |
N/A |
Umbilical region |
Discharge |
0.5 |
Punch excision |
Secondary intention |
No recurrence |
2 |
|
Dhalani et al./ 2025 [2] |
35 |
M |
Recurrent PNS & polycythemia vera |
N/A |
Natal cleft |
Pain & discharge |
0.16 |
Excision of sinus tract |
Secondary intention, Leech therapy & turmeric powder |
No recurrence |
2 |
|
Anand et al./2022 [10] |
10 |
M |
Unremarkable |
Unremarkable |
Left preauricular region |
Discharge |
10 |
Excision of sinus tract |
Sterile dressing |
No recurrence |
N/A |
|
Salih et al./ 2022 [4] |
27 |
M |
Unremarkable |
Unremarkable |
Posterior aspect of the auricle |
Discharge |
13 |
Excision of sinus tract |
Kurdish gum |
No recurrence |
N/A |
|
Othman et al./2022 [8] |
62 |
M |
Unremarkable |
Unremarkable |
Umbilical region |
Pain & discharge |
N/A |
Excision of sinus tract |
Not mentioned |
No recurrence |
N/A |
|
Mirande et al./2022 [3] |
13 |
F |
Obesity |
Unremarkable |
Intermammary region |
Discharge |
1 |
Wide local excision sinus tract |
Not mentioned |
No recurrence |
0.2 |
|
Adhikari et al/ 2021[7] |
37 |
M |
Recurrent discharging sinus |
N/A |
Bulge of the cheek |
Discharge |
2 |
Wide excision of the sinuses |
Not mentioned |
No recurrence |
1.5 |
|
Salih et al./2020 [11] |
25 |
F |
Unremarkable |
N/A |
Bilateral Inframammary region |
Discharge and induration |
2 |
Excision of sinus tract |
Not mentioned |
No recurrence |
0.5 |
|
Deshpande et al./ 2020[12] |
22 |
F |
Unremarkable |
Unremarkable |
Intermammary region |
Discharge |
1 |
Excision of sinus tract & laser epilation |
Silicone dressing |
No recurrence |
0.5 |
|
M: male, F: female, N/A: non-applicable, PNS: Pilonidal sinus, Y: Years |
|||||||||||
Most cases of IMPNS present with induration in the intermammary region, an abscess, or a sinus opening with spontaneous discharge. Although the current patient was not obese, some studies suggest a higher incidence of IMPNS in obese individuals [1]. Mirande et al. reported a case of a young girl with a history of obesity (BMI: 33.13) who developed recurrent IMPNS, further supporting a possible link between obesity and this condition [3]. While obesity has not been explicitly identified as a risk factor in the literature, its potential contribution warrants further investigation. Although there is no standardized management strategy for IMPNS, definitive treatment, similar to NCPNS, typically involves excision and primary closure to achieve an optimal cosmetic outcome. Incomplete excision of all sinus tracts in IMPNS is associated with a high recurrence rate [1]. In the current case, the patient was successfully treated with sinus tract extraction, resulting in complete resolution.
Umbilical discharge is uncommon in adults, especially in the absence of prior surgical history. The primary differential diagnoses include UPNS, urachal remnants, and omphalomesenteric duct remnants [8]. In the current case, the latter two were considered unlikely, as the patient did not exhibit typical signs such as urine leakage from the umbilicus, persistent moisture or irritation, or feculent discharge. The primary risk factors for UPNS are similar to other types of PNS, including male gender and hirsutism, particularly when hair growth directs loose hairs toward the umbilicus. Additional contributing factors include a deep navel and, to a lesser extent, obesity, neither of which was present in the current patient [9]. Hassan et al. stated that conservative treatment of UPNS can be effective, as demonstrated in the current patient, who was treated with hair removal and daily povidone-iodine dressing [13]. According to Savant, the recurrence rate of UPNS is minimal, and the procedure can be easily repeated if needed. Combining it with laser hair removal may further lower recurrence rates and help prevent new lesions [9].
Non-operative management plays a limited role in NCPNS, as surgical excision is typically required. Treatment options include excision with primary closure or excision with secondary healing, where the wound is left open to heal naturally [4]. Lord’s procedure was deemed appropriate as there were no signs of extensive inflammation or abscess formation, making it suitable for a tissue-sparing approach.
Conclusion
In conclusion, the simultaneous presentation of NCPNS, UPNS, and IMPNS is extremely rare. A surgical approach for NCPNS and IMPNS, combined with a conservative approach for UPNS, may lead to favorable outcomes.
Declarations
Conflicts of interest: The authors have no conflicts of interest to disclose.
Ethical approval: Not applicable.
Consent for participation: Not applicable.
Consent for publication: Written informed consent for publication was obtained from the patient.
Funding: The present study received no financial support.
Acknowledgments: None to be declared.
Authors' contributions: ESS, SHH, and MMA: Major contributors to the conception of the study, as well as the literature search for related studies, and manuscript writing. AAQ, IHQ, and KZH: Literature review, critical revision of the manuscript, and processing of the tables and figures. All authors have read and approved the final version of the manuscript.
Use of AI: ChatGPT-3.5 was used to assist with language refinement and improve the overall clarity of the manuscript. All content was thoroughly reviewed and approved by the authors, who bear full responsibility for the final version.
Data availability statement: Not applicable.